ACCL0933
A Randomized Open-Label Trial of Caspofungin versus Fluconazole to Prevent Invasive Fungal Infections in Children Undergoing Chemotherapy for Acute Myeloid Leukemia (AML)
A Groupwide Phase III Study
THIS PROTOCOL IS FOR RESEARCH PURPOSES ONLY, AND SHOULD NOT BE COPIED, REDISTRIBUTED OR USED FOR ANY OTHER PURPOSE. MEDICAL AND SCIENTIFIC INFORMATION CONTAINED WITHIN THIS PROTOCOL IS NOT INCLUDED TO AUTHORIZE OR FACILITATE THE PRACTICE OF MEDICINE BY ANY PERSON OR ENTITY. RESEARCH means a systematic investigation, including research development, testing and evaluation, DESIGNED TO DEVELOP OR CONTRIBUTE TO GENERALIZABLE KNOWLEDGE. THIS PROTOCOL IS THE RESEARCH PLAN DEVELOPED BY THE CHILDREN'S ONCOLOGY GROUP TO INVESTIGATE A PARTICULAR STUDY QUESTION OR SET OF STUDY QUESTIONS AND SHOULD NOT BE USED TO DIRECT THE PRACTICE OF MEDICINE BY ANY PERSON OR TO PROVIDE INDIVIDUALIZED MEDICAL CARE, TREATMENT, OR ADVICE TO ANY PATIENT OR STUDY SUBJECT. THE PROCEDURES IN THIS PROTOCOL ARE INTENDED ONLY FOR USE BY CLINICAL ONCOLOGISTS IN CAREFULLY STRUCTURED SETTINGS, AND MAY NOT PROVE TO BE MORE EFFECTIVE THAN STANDARD TREATMENT. ANY PERSON WHO REQUIRES MEDICAL CARE IS URGED TO CONSULT WITH HIS OR HER PERSONAL PHYSICIAN OR TREATING PHYSICIAN OR VISIT THE NEAREST LOCAL HOSPITAL OR HEALTHCARE INSTITUTION.
TABLE OF CONTENTS
SECTION ..... PAGE
STUDY COMMITTEE ..... 4
ABSTRACT ..... 6
EXPERIMENTAL DESIGN SCHEMA ..... 7
1.0 GOALS AND OBJECTIVES (SCIENTIFIC AIMS) ..... 8
1.1 Primary Objective ..... 8
1.2 Secondary Objectives ..... 8
2.0 BACKGROUND ..... 8
2.1 Overview and Rationale for Study ..... 8
2.2 Selection of Study Medication ..... 9
2.3 Rationale for Platelia EIA Aspergillus GM and Serum Beta-D Glucan Assays ..... 12
3.0 STUDY ENROLLMENT AND PATIENT ELIGIBILITY ..... 13
3.1 Study Enrollment ..... 13
3.2 Patient Eligibility Criteria ..... 14
4.0 TREATMENT PLAN ..... 16
4.1 Overview of Treatment Plan ..... 16
4.2 Administration Schedule- FLUCONAZOLE ARM ..... 18
4.3 Administration Schedule- CASPOFUNGIN ARM ..... 20
5.0 DOSE MODIFICATIONS FOR TOXICITIES ..... 22
5.1 Impaired Renal Function ..... 22
5.2 Impaired Liver Function ..... 22
6.0 DRUG INFORMATION ..... 23
6.1 FLUCONAZOLE (Diflucan ) ..... 23
6.2 CASPOFUNGIN (caspofungin acetate, Cancidas ) (11/08/11) ..... 26
7.0 EVALUATIONS/MATERIAL AND DATA TO BE ACCESSIONED ..... 29
7.1 Required and Optional Clinical, Laboratory and Disease Evaluations ..... 29
7.2 Optional Studies ..... 30
7.3 Follow-up ..... 30
8.0 CRITERIA FOR REMOVAL FROM PROTOCOL THERAPY AND OFF STUDY CRITERIA ..... 30
8.1 Criteria for Removal from Protocol Therapy ..... 30
8.2 Off Study Criteria ..... 30
8.3 Discontinuation from IFI Observation Criteria ..... 31
9.0 STATISTICAL CONSIDERATIONS ..... 31
9.1 Statistical Design ..... 31
9.2 Patient Accrual and Expected Duration of Trial ..... 31
9.3 Statistical Analysis Methods ..... 31
9.4 Gender and Minority Accrual Estimates ..... 35
10.0 EVALUATION CRITERIA ..... 36
10.1 Common Terminology Criteria for Adverse Events (CTCAE) ..... 36
10.2 IFI Checklist and Central Review ..... 36
11.0 ADVERSE EVENT REPORTING REQUIREMENTS ..... 36
11.1 Purpose ..... 36
11.2 Determination of Reporting Requirements ..... 37
11.4 Routine Adverse Event Reporting ..... 38
12.0 RECORDS AND REPORTING ..... 38
12.1 CDUS ..... 38
13.0 PROSPECTIVE EVALUATION OF GALACTOMANNAN AND ( ) BETA-D GLUCAN ASSAYS AS DIAGNOSTIC TOOLS FOR INVASIVE FUNGAL INFECTION IN CHILDREN WITH ACUTE MYELOID LEUKEMIA RECEIVING FUNGAL PROPHYLAXIS. ..... 39
13.1 Sample Collection and Testing Procedures (These studies are optional) ..... 39
13.2 Background ..... 42
13.3 Specific Aims ..... 45
13.4 Patient Accrual ..... 45
13.5 Gold Standards for IFI and IA Infections ..... 46
13.6 Methodology to Identify IFI and IA ..... 46
13.7 Factors resulting in False Positive Results ..... 47
13.8 Statistical Design ..... 47
13.9 Significance ..... 49
14.0 SPECIAL STUDIES SPECIMEN REQUIREMENTS ..... 50
14.1 Single Nucleotide Polymorphisms (This study is optional) ..... 50
15.0 BANKING SPECIMENS ..... 50
APPENDIX I: YOUTH INFORMATION SHEETS ..... 51
APPENDIX II: EORTC/MSG CRITERIA ..... 53
REFERENCES ..... 55
SAMPLE RESEARCH INFORMED CONSENT/PARENTAL PERMISSION FORM ..... 59
The Children's Oncology Group has received a Certificate of Confidentiality from the federal government, which will help us protect the privacy of our research subjects. The Certificate protects against the involuntary release of information about subjects collected during the course of our covered studies. The researchers involved in the studies cannot be forced to disclose the identity or any information collected in the study in any legal proceedings at the federal, state, or local level, regardless of whether they are criminal, administrative, or legislative proceedings. However, the subject or the researcher may choose to voluntarily disclose the protected information under certain circumstances. For example, if the subject or his/her guardian requests the release of information in writing, the Certificate does not protect against that voluntary disclosure. Furthermore, federal agencies may review our records under limited circumstances, such as a DHHS request for information for an audit or program evaluation or an FDA request under the Food, Drug and Cosmetics Act. The Certificate of Confidentiality will not protect against mandatory disclosure by the researchers of information on suspected child abuse, reportable communicable diseases, and/or possible threat of harm to self or others.
Abstract
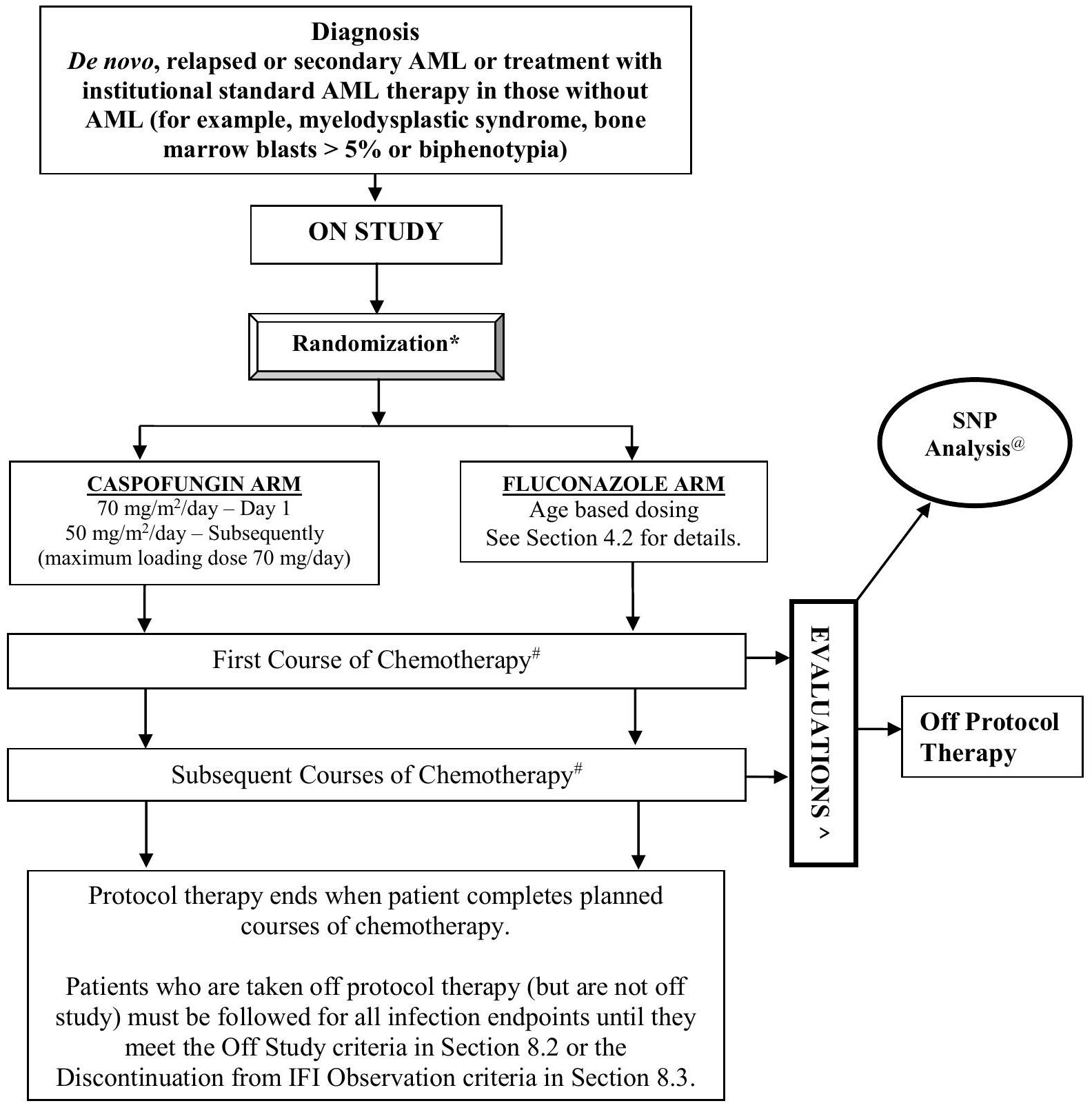
Invasive fungal infections (IFI) have steadily increased over the past 2 decades in children with acute myeloid leukemia (AML). Over 50% of infectious-related deaths in this population are attributable to IFI. These dismal numbers are despite empiric therapy and treatment with the best available agents. The failure of these strategies to impact morbidity and mortality from IFI makes a strong case for the exploration of preventive strategies. This study will utilize a 2 -arm, open-label randomized design to evaluate the efficacy of prophylaxis with caspofungin in comparison with fluconazole in children with de novo, relapsed or secondary AML. Study agent will begin following completion of each course of chemotherapy and continue through periods of neutropenia. This study also seeks to evaluate the usefulness of the Platelia EIA Aspergillus galactomannan (GM) assay as well as beta-D glucan testing in early diagnosis of IFI. ACCL0933 will also explore the relationship between proven or probable IFI and single nucleotide polymorphisms (SNP) of genes involved in immunity and develop predictive models of IFI that will be useful in the early identification of susceptible patients.
EXPERIMENTAL DESIGN SCHEMA
1.0 GOALS AND OBJECTIVES (SCIENTIFIC AIMS)
1.1 Primary Objective
1.1.1
To determine if prophylaxis with caspofungin administered during periods of neutropenia following chemotherapy for acute myeloid leukemia (AML) is associated with a lower incidence of proven or probable invasive fungal infections (IFI) compared with fluconazole.
1.2 Secondary Objectives
Clinical
1.2.1
To determine if prophylaxis with caspofungin will result in a lower incidence of proven or probable cases of invasive aspergillosis (IA) compared with fluconazole.
1.2.2
To determine if prophylaxis with caspofungin will result in improved survival compared to fluconazole.
1.2.3
To determine if prophylaxis with caspofungin will result in less empiric antifungal therapy compared to fluconazole.
Biological
1.2.4
To determine the sensitivity, specificity, positive and negative predictive value of biweekly galactomannan (GM) and beta-D glucan testing in diagnosing IFI.
1.2.5
To test the association between single nucleotide polymorphisms (SNPs) in genes involved in innate immunity and proven or probable IFI.
1.2.6
To develop predictive models of IFI using SNP in genes involved in immunity and clinical covariates.
2.0 BACKGROUND
2.1 Overview and Rationale for Study
This study is a 2 -arm open-label randomized clinical trial to evaluate the efficacy of caspofungin prophylaxis compared with fluconazole prophylaxis. A total of approximately 550 subjects will be randomized (until accrual of at least 275 participants on each treatment arm) during periods of neutropenia associated with chemotherapy for the treatment of AML.
The frequency and severity of IFI in immunocompromised patients has increased steadily over the past 2 decades. The incidence of IFI as a cause of sepsis has more than tripled with 5,231 cases in 1979 compared with 16,042 cases in In children with fungal sepsis, the case fatality rate has been estimated to be Among children with cancer, those undergoing hematopoietic stem cell transplantation (HSCT) and those receiving AML therapy are at highest risk for IFI. The most common
causes of IFI in children with cancer are Candida spp. and Aspergillus spp.
Candida spp. are commensal organisms that normally reside on mucosal and skin surfaces. The portal of entry is typically the gut mucosa and less commonly the skin. Therefore, children undergoing intensive therapy for cancer that results in mucositis are at high risk for infection with Candida spp. Although mucosal candidal infections occur, candidemia is the most serious clinical syndrome caused by Candida spp. Its manifestations may include fever unresponsive to antibiotics, macronodular skin lesions, myalgias, and sepsis. Acute hematogenous dissemination of Candida to 1 or more organs can occur including the heart, lung, brain, eye, kidney, liver and spleen. Immunocompromised children are at higher risk for disseminated disease. Disseminated infections are considered to be more severe and require longer courses of antifungal therapy. The attributable mortality of invasive candidiasis in children has been reported to be . These data suggest that 1 child would be saved for every 10 children in whom candidemia can be prevented.
Infections with Aspergillus spp. account for the vast majority of non-Candida IFI in children with cancer. Children undergoing AML therapy have the highest risk of IA outside the transplant setting. IA most commonly presents as pneumonia. Infiltrates are commonly wedge-shaped, pleural-based or nodular and visible on chest radiographs or CT scans. The infiltrates may initially be accompanied by a halo sign and later by a crescent sign. In children with uncontrolled infection, the infiltrates may be diffuse. Less commonly, sinusitis may also occur. Finally, Aspergillus can disseminate to the central nervous system. IA is associated with mortality rates in children of greater than
The burden of IFI in pediatric AML is considerable. CCG 2961 demonstrated that the incidence of IFI in children with AML was per treatment phase. Approximately half the infections were caused by Aspergillus and the other half by Candida. Most importantly, of infection-related deaths were associated with Aspergillus, and 25.9% of infectious deaths were associated with Candida. In order to impact on survival of children with AML, strategies to reduce IFI are urgently needed. In general, the 3 types of strategies directed toward fungal infections are prophylaxis, empiric therapy, and treatment of IFI. The current rates of IFIs and attributable mortality due to IFI are primarily derived from the setting of empiric therapy and treatment with best available agents, and thus, these strategies currently are insufficient to make a major impact on fungal morbidity and mortality. Thus, strategies to prevent IFI should be the priority. Furthermore, IFIs likely impact on the ability to deliver anti-leukemic therapy and many IFI are never microbiologically documented, further strengthening the imperative to prevent IFI rather than relying upon empiric or treatment strategies alone.
2.2 Selection of Study Medication
2.2.1 Choice of Fluconazole Prophylaxis as the Standard Arm
A systematic review and meta-analysis of randomized, clinical trials demonstrated antifungal prophylaxis significantly decreased all-cause mortality in patients receiving chemotherapy. The conclusions from the systematic review and consensus guidelines from the Centers for Disease Control and Prevention, the Infectious Disease Society of America, the American Society for Blood and Marrow Transplantation, and the first European Conference on Infections in Leukemia all recommend antifungal prophylaxis for HSCT recipients. The systematic review concluded that antifungal prophylaxis "should probably be administered to high-risk leukemia patients."
Fluconazole has been shown to be an effective antifungal agent for prophylaxis against IFI in high-risk patients in previous studies and antifungal prophylaxis with fluconazole reduces morbidity and mortality among allogeneic HSCT recipients. Fluconazole has also been used in other patient populations with neutropenia, although its effectiveness in these patients is less clear. However, fluconazole may not be
the best agent for patients with AML since it lacks activity against filamentous fungi (e.g. Aspergillus), which represent half the causes of IFI in children with AML.
Nonetheless, the trial uses fluconazole as the standard prophylaxis arm because it is effective against Candida infections, and its use as prophylaxis is regarded appropriate by the above mentioned consensus guidelines. The first European Conference on Infections in Leukemia, published in 2007, recommended fluconazole as the preferred agent for anti-fungal prophylaxis. In addition, as highlighted by Wingard, it is not known whether the toxicity and cost of adding empiric mold coverage is superior to a strategy of fluconazole and aggressive monitoring and pre-emptive treatment for molds.
Furthermore, fluconazole was chosen as the comparator as it is the most commonly used agent for antifungal prophylaxis in pediatric AML in North America and according to a recent COG-wide survey, 154/178 ( ) of institutions currently use either fluconazole or no prophylaxis in children with de novo AML.
Another possible agent which could have been chosen as the control arm is itraconazole. Itraconazole has a wider spectrum of activity than fluconazole, including activity against Aspergillus and has been shown to be more effective than fluconazole when used for prophylaxis in patients with neutropenia. However, the clinical usefulness of itraconazole is limited by poor tolerability and bioavailability of the oral formulations.
2.2.2 Choice of Caspofungin Prophylaxis as the Intervention Arm
Newer antifungal agents with a broader spectrum of activity that have been considered as study medications include the newer azoles (voriconazole, posaconazole) and the echinocandins (caspofungin, micafungin, anidulafungin). The following highlights why caspofungin was chosen as the intervention arm.
2.2.2.1 Azole Antifungal Agents
The broad-spectrum azoles, including voriconazole and posaconazole, have in vitro activity against a wide spectrum of fungi including Candida and Aspergillus.
Voriconazole is Food and Drug Administration (FDA) approved for the treatment of aspergillosis and candidiasis. There are two studies that have compared voriconazole to fluconazole or itraconazole for prophylaxis. A randomized, double-blind trial of fluconazole vs. voriconazole for the prevention of IFI in 600 HSCT patients was conducted. The primary endpoint was fungal free survival rate at 6 months and this survival was in the fluconazole group and in the voriconazole group ( ). Overall survival was , respectively. The incidence of fungal infection was not statistically different and was in the fluconazole arm and in the voriconazole arm ( ). Another study compared voriconazole vs. itraconazole in 114 adult high-risk leukemia patients. Two patients in the itraconazole group and no patients in the voriconazole group developed an IFI. However, the numbers were too small for a meaningful statistical comparison. Response to chemotherapy, overall mortality and survival were similar in both groups. Of particular significance, of patients receiving voriconazole discontinued prophylaxis due to side effects compared to of patients receiving itraconazole. All of these studies were conducted in adults.
In addition to the prophylactic setting, it may also be useful to examine voriconazole in the empiric antifungal setting as it may shed insight into its efficacy. Voriconazole was compared to liposomal amphotericin B for empiric antifungal therapy in patients with neutropenia and persistent fever. This was a large, randomized trial that included over 800 patients. The overall success rates were for voriconazole and for liposomal amphotericin B ( confidence interval for the difference, -10.6 to 1.6). Thus, voriconazole failed the non-inferiority cut-off, suggesting that voriconazole may be inferior
to liposomal amphotericin B for empiric treatment of fever and neutropenia raising questions about its efficacy in patients with febrile neutropenia.
The largest pediatric study of voriconazole was an open label, compassionate-use evaluation in 58 children with proven or probable IFI refractory to or intolerant of conventional antifungal therapy. Forty-five percent of the patients had a complete or partial response to therapy.
Metabolism of voriconazole occurs in the liver via CYP450 enzyme family, including CYP2C9, CYP3A4, and CYP2C19 isoenzymes and therefore, the potential for drug interactions with voriconazole is high. The main side effects of voriconazole include visual disturbances, skin rashes, elevations in hepatic enzymes and rarely, severe, life-threatening hepatitis.
When evaluating studies of antifungal agents with anti-mold activity vs. fluconazole, there are three trials that showed improved survival and/or a lower rate of IFI when anti-mold agents were compared to fluconazole. Two of the studies used posaconazole and one trial used micafungin. In other words, there are no studies that have demonstrated that voriconazole is superior to fluconazole as prophylaxis against IFI. Therefore, the decision not to use voriconazole as the comparator in this trial was based on available data that show no significant advantage over fluconazole or itraconazole, the potential for toxicity, and the potential for drug interactions in children receiving AML chemotherapy. Furthermore, pharmacokinetics and appropriate dosing are less certain in children compared with adults, thus making voriconazole even less attractive in this population.
Posaconazole is an attractive agent to consider as antifungal prophylaxis in the AML population. A randomized, multi-center study of posaconazole vs. fluconazole or itraconazole in patients with neutropenia associated with the treatment of AML or myelodysplastic syndrome found that posaconazole reduced the rate of IFI from to compared to fluconazole. However, children less than 13 years of age were excluded and the median age of study subjects was approximately 50 years of age. Its use is limited in children because of insufficient dosing information for young children. Furthermore, posaconazole has the same concerns regarding hepatotoxicity and drug interactions as exist for voriconazole. Finally, posaconazole can only be administered as an oral agent currently and children receiving AML therapy may not be able to comply with oral medication during the neutropenic period. Therefore, posaconazole is not an appropriate agent to use in children with AML at this time.
The next COG Phase 3 AML trial will randomize subjects to receive or not receive bortezomib and there is considerable risk of drug interactions with concurrent administration of bortezomib and either voriconazole or posaconazole, thus further decreasing the feasibility of their use in pediatric AML.
2.2.2.2 Echinocandin Antifungal Agents
Echinocandins target cell wall biosynthesis of -1, 3-glucan and exhibit in vitro activity against both Candida and Aspergillus species. There are 3 currently available echinocandins, namely micafungin, anidulofungin and caspofungin.
Micafungin has been studied in children with cancer. A Phase I pediatric febrile neutropenia study found that doses up to day IV were well tolerated with no side effects. A recent study of micafungin in combination with a second antifungal agent in pediatric and adult bone marrow recipients with IA revealed an overall response rate of The success rate in the pediatric patient population was similar to the adult patients. Pediatric patients were also enrolled in a recent micafungin prophylaxis study in patients undergoing HSCT. This study was a randomized, double-blind, multi-center study of 882 patients, of which were children younger than 16 years of age. Although the study did not have statistical power to specifically address efficacy in the pediatric subgroup, the magnitude and the direction of micafungin efficacy were similar in children and adults. Dosing in children under the age of 8 years
appears to yield a higher clearance of micafungin, resulting in the likely need for an increased dose in this age group. Despite the pharmacokinetic studies and its recent FDA approval in adults, there is no accepted dosage of micafungin in pediatric patients.
Anidulafungin has the least data in pediatric patients. A Phase I/II dose escalation study of anidulafungin in children with persistent neutropenia showed that the drug was well tolerated in pediatric patients and can be dosed based on body weight. Pediatric patients receiving 0.75 or IV have pharmacokinetic properties similar to adults receiving day, respectively.
Among the echinocandins, caspofungin is the most extensively studied agent in children. Caspofungin recently received FDA approval for use in children months of age. There have been 5 pediatric caspofungin studies ( 3 pharmacokinetic and 2 safety/efficacy trials). A multicenter, prospective, openlabel study in 50 children with proven candidiasis or aspergillosis was recently completed. Caspofungin was well-tolerated. Fifty percent of children with IA and of children with invasive candidiasis were successfully treated. These efficacy outcomes were consistent with previous adult studies focused on these infections. A randomized, double-blind, multicenter trial of caspofungin vs. liposomal amphotericin for empirical antifungal therapy of pediatric patients with persistent fever and neutropenia was also completed. Overall success rates were for caspofungin vs. for liposomal amphotericin; however, this difference did not reach statistical significance. Caspofungin demonstrated efficacy consistent with adult data for this indication. A comprehensive review of the safety of caspofungin across the 5 pediatric studies was performed. Of the 171 children receiving caspofungin, therapy was discontinued due to drug-related adverse events in 3 patients. Elevations in serum transaminases were seen in of patients. The currently recommended pediatric dose of caspofungin in children is day IV on the first day of therapy followed by day IV for subsequent days. The maximum daily loading dose is 70 mg . The maximum daily maintenance dose is 50 mg .
Based on the available dosing data, safety data, and efficacy data regarding the echinocandins, caspofungin has been chosen as the best suited agent to take forward into studies of antifungal prophylaxis in pediatric AML patients because it is the only echinocandin approved for use in children as young as 3 months of age and because of extensive experience in children with cancer. Furthermore, there have been safety concerns raised recently regarding the use of micafungin in children from the European Medicines Agency. Finally, there is no approved dosing for anidulofungin in young children.
2.3 Rationale for Platelia EIA Aspergillus GM and Serum Beta-D Glucan Assays
The diagnosis of IFI, especially IA, is often difficult because of the lack of specific clinical symptoms in high-risk patients and the invasiveness of standard diagnostic tests. Therefore much attention has been focused on developing non-invasive tests for diagnosing IFI. GM is a polysaccharide cell-wall component that is released by Aspergillus during growth. The Platelia EIA Aspergillus GM assay was approved by the FDA in 2003 for use in adult patients. Early large scale clinical testing included few children, but available data suggest that detection values for adult patients may not be extrapolated to children. Furthermore, the utility of the GM assay in pediatric patients has not been rigorously studied in a prospective manner and therefore its true value as a diagnostic test in children is still unclear. Serum betaD glucan (found in all fungi except Cryptococcus species and Zygomycetes) can be detected using an approved diagnostic serum assay and has been found to have high specificity and high positive predictive values for the detection of IFI in adults. However, data on the performance of this assay in children are limited. Data suggests that combining GM testing with beta-D glucan testing would further improve the usefulness of the test; twice weekly testing having been suggested as practical to enable reasonably prompt diagnosis of IFI. See Section 13 for details on these optional ancillary studies.
2.4 Rationale for Single Nucleotide Polymorphism (SNP) Aim
In addition to early detection of fungal infections, there also is interest in identifying children particularly susceptible to these infections. There is considerable evidence that there is a genetic component to the susceptibility and outcome of infection in both normal and immunocompromised populations. For example, a study using a Danish adoption registry found that premature death from infection is much more heritable compared to premature death from cardiovascular disease or cancer. Redundancy in the immune system may be important for protection against serious infection and in the face of immunosuppression, defects in redundant pathways may be uncovered, leading to invasive bacterial or fungal infections. While defects in immunity may contribute to susceptibility to infection and outcome, excessive inflammation during infection may also contribute to septic shock and mortality. Thus, variation in immunity and inflammatory genes likely plays a role in an individual's susceptibility, response and prognosis related to infection. There is evidence specifically to link SNPs and the risk of fungal infections. For example, Choi and colleagues found that 2 polymorphisms in IL-4 were associated with chronic disseminated candidiasis in patients with acute leukemia. In addition, a polymorphism in DEF was associated with Candida carriage in type 1 diabetes. Based on these and other studies, we propose to test for associations between genetic variants in genes mediating innate immunity and IFI.
3.0 STUDY ENROLLMENT AND PATIENT ELIGIBILITY
3.1 Study Enrollment
3.1.1 Patient Registration
Prior to enrollment on this study, patients must be assigned a COG patient ID number. This number is obtained via the eRDE system once authorization for the release of protected health information (PHI) has been obtained. The COG patient ID number is used to identify the patient in all future interactions with COG. If you have problems with the registration, please refer to the online help.
In order for an institution to maintain COG membership requirements, every newly diagnosed patient needs to be offered participation in ACCRN07, Protocol for the Enrollment on the Official COG Registry, The Childhood Cancer Research Network (CCRN).
A Biopathology Center (BPC) number will be assigned as part of the registration process. Each patient will be assigned only one BPC number per COG Patient ID. For additional information about the labeling of specimens please refer to the Pathology and/or Biology Guidelines in this protocol.
3.1.2 IRB Approval
Local IRB/REB approval of this study must be obtained by a site prior to enrolling patients. Sites must submit IRB/REB approvals to the NCI's Cancer Trials Support Unit (CTSU) Regulatory Office and allow 3 business days for processing. The submission must include a fax coversheet (or optional CTSU IRB Transmittal Sheet) and the IRB approval document(s). The CTSU IRB Certification Form may be submitted in lieu of the signed IRB approval letter. All CTSU forms can be located on the CTSU web page (https://www.ctsu.org). Any other regulatory documents needed for access to the study enrollment screens will be listed for the study on the CTSU Member's Website under the RSS Tab.
IRB/REB approval documents may be faxed (1-215-569-0206) Emailed
(CTSURegulatory@ctsu.coccg.org) or mailed to the CTSU Regulatory office.
When a site has a pending patient enrollment within the next 24 hours, this is considered a "Time of Need" registration. For Time of Need registrations, in addition to marking your submissions as 'URGENT' and faxing the regulatory documents, call the CTSU Regulatory Helpdesk at: 1-866-651CTSU. For general (non-regulatory) questions call the CTSU General Helpdesk at: 1-888-823-5923.
3.1.3 Study Enrollment
Patients may be enrolled on the study once all eligibility requirements for the study have been met. Study enrollment is accomplished by going to the Enrollment application in the RDE system. If you have problems with enrollment, refer to online help in the Applications area of the COG website.
3.1.4 Timing
Patients must be enrolled before protocol-directed antifungal prophylaxis begins. Treatment with nonprotocol directed antifungal prophylaxis with any agent is permitted prior to enrollment, but treatment with fluconazole or caspofungin (determined by randomization at enrollment) starts within 24-72 hours following completion of the first course of current chemotherapy. The date protocol-directed antifungal prophylaxis is projected to start must be no later than 5 calendar days after the date of study enrollment however, consent may be obtained earlier, and may occur at the same time consent is obtained for AML treatment.
All clinical and laboratory studies to determine eligibility must be performed within 7 days prior to enrollment unless otherwise indicated in the eligibility section below.
3.1.5 Bilingual Services
To allow non-English speaking patients to participate in the study, bilingual health care services will be provided in the appropriate language.
3.1.6 Randomization
Randomization will take place at the time a patient is entered On Study via RDE. Patients will be assigned to either antifungal prophylaxis with caspofungin or antifungal prophylaxis with fluconazole. Randomization will be stratified into 2 groups: 1) de novo AML vs. 2) all other patients.
3.2 Patient Eligibility Criteria
Important note: The eligibility criteria listed below are interpreted literally and cannot be waived (per COG policy 7.2). All clinical and laboratory data required for determining eligibility of a patient enrolled on this trial must be available in the patient's medical/research record which will serve as the source document for verification at the time of audit.
INCLUSION CRITERIA
3.2.1 Age
Patients must be months and years at the time of enrollment.
3.2.2 Diagnosis
Patients must have one of the following diagnoses and/or treatment plans:
Newly diagnosed de novo AML
First or subsequent relapse of AML
Secondary AML
Treatment with institutional standard AML therapy in those without AML (for example myelodysplastic syndrome, bone marrow blasts > 5% or biphenotypia).
Please note: Patients with a history of prolonged antifungal therapy (example relapsed AML) are eligible.
3.2.3 Organ Function Requirements:
3.2.3.1 Adequate renal function defined as:
Creatinine clearance or radioisotope GFR
A serum creatinine based on age/gender as follows:
Age
Maximum Serum Creatinine (mg/dL)
Male
Female
1 month to < 6 months
0.4
0.4
6 months to < 1 year
0.5
0.5
1 to < 2 years
0.6
0.6
2 to < 6 years
0.8
0.8
6 to < 10 years
1
1
10 to < 13 years
1.2
1.2
13 to < 16 years
1.5
1.4
years
1.7
1.4
The threshold creatinine values in this Table were derived from the Schwartz formula for estimating GFR utilizing child length and stature data published by the CDC.
3.2.3.2 Adequate liver function defined as:
Total bilirubin upper limit of normal (ULN) for age, and
SGOT (AST) or SGPT (ALT) ULN for age.
EXCLUSION CRITERIA
3.2.4 Patients with the following diagnoses are not eligible:
acute promyelocytic leukemia (APL)
Down syndrome
juvenile myelomonocytic leukemia (JMML)
3.2.5 Patients with a documented history of IFI within the previous 30 days are not eligible.
3.2.6 Patients with a history of echinocandin or fluconazole hypersensitivity are not eligible.
3.2.7 Patients receiving treatment for an IFI are not eligible.
3.2.8 Female patients of childbearing age must have a negative pregnancy test. Patients must agree to use an effective birth control method. Lactating patients must agree not to nurse a child while on this trial.
REGULATORY
3.2.9 All patients and/or their parents or legal guardians must sign a written informed consent.
3.2.10 All institutional, FDA, and NCI requirements for human studies must be met.
4.0 TREATMENT PLAN
Timing of protocol therapy administration, response assessment studies, and surgical interventions are based on schedules derived from the experimental design or on established standards of care. Minor unavoidable departures (up to 72 hours) from protocol directed therapy and/or disease evaluations (and up to 1 week for surgery) for valid clinical, patient and family logistical, or facility, procedure and/or anesthesia scheduling issues are acceptable per COG administrative Policy 5.14 (except where explicitly prohibited within the protocol).
4.1 Overview of Treatment Plan
This is a randomized clinical trial designed to assess the efficacy of caspofungin for preventing IFI (including IA) compared to fungal prophylaxis with fluconazole, the standard of therapy used in most COG institutions as prophylaxis in patients with AML and chemotherapy-induced neutropenia.
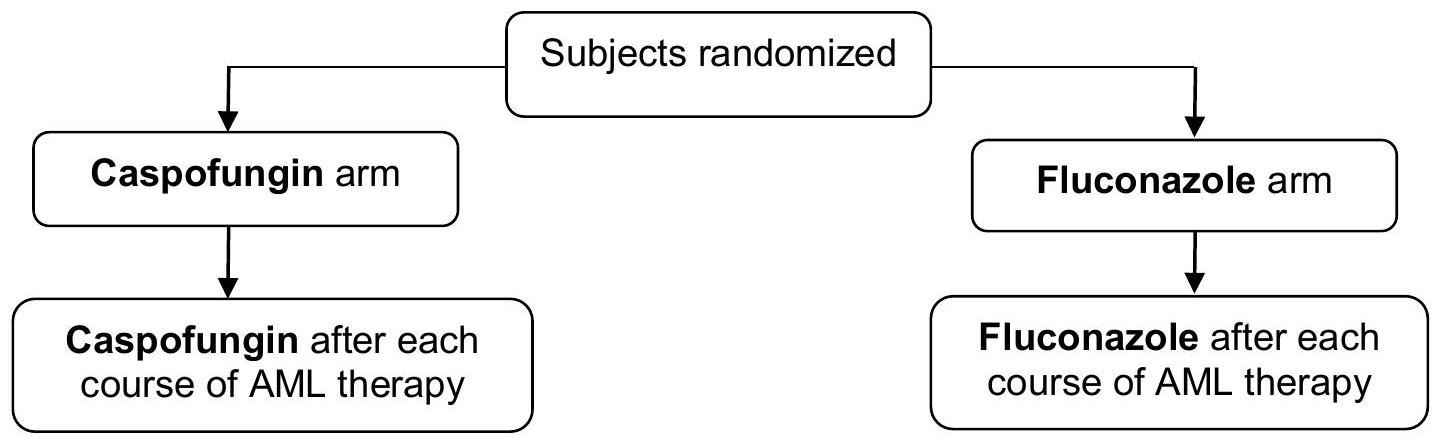
Patients who consent to participate in ACCL0933 will be randomly assigned to antifungal prophylaxis with either fluconazole or caspofungin. Treatment with any anti-fungal prophylaxis after enrollment must be terminated prior to starting protocol-directed anti-fungal therapy. Protocol prophylaxis will be started within 24-72 hours following the last dose of systemic chemotherapy for each course. Administration of antifungal prophylaxis for each course will continue until (a) The absolute neutrophil count (ANC) is following the nadir; (b) Start of the next chemotherapy course; (c) Patient meets any off-protocol criteria (Section 8.1).
If other systemic antifungal therapy is initiated for empiric therapy or treatment of suspected infection, then protocol prophylaxis should be held and assigned prophylaxis should resume when other systemic antifungal therapy is discontinued if this occurs prior to ANC recovery.
Administration of assigned systematic antifungal prophylaxis continues with subsequent courses of chemotherapy until the patient meets any off-protocol criteria including proven or probable IFI according to institutional diagnosis.
Fluconazole may be administered either intravenously (IV) or orally. Caspofungin is only available as an IV formulation.
Note - For those institutions where patients are discharged prior to ANC recovery to the following options exist:
If the patient has been randomized to fluconazole they can continue this therapy orally at home until the ANC is .
If the patient is on caspofungin the parents and patient can decide to either remain in the hospital to continue caspofungin until the ANC is or be discharged home on daily IV caspofungin therapy until the ANC is . The latter may be associated with home healthcare costs that would not be funded by the study. It should be confirmed prior to discharge that the insurance company or other sources will cover such home healthcare costs.
If the insurance company or other sources will not cover home healthcare costs not funded by the study, then the family can elect to pay for these services themselves or go home without continued caspofungin prophylaxis. In this circumstance, the treating physician should proceed with their standard clinical practices.
See Section 6.2 for information regarding investigational vs. commercial drug supply following discharge home.
4.1.1. Randomization
At the time of enrollment, patients will be randomly assigned to one of two treatment regimens:
i) Fluconazole Arm: This group will receive fluconazole, and represents the standard arm.
ii) Caspofungin Arm: This group will receive caspofungin and represents the experimental arm.
Randomization will be stratified into 2 groups: 1) de novo AML vs. 2) all other patients.
4.1.2 Empirical Antifungal Therapy
The persistence of fever for 5 days despite broad spectrum antibiotic therapy warrants the investigation of IFI and initiation of empiric antifungal therapy. Amphotericin B (lipid products) or voriconazole are recommended options based on their broad spectrum of antifungal activity. Assigned antifungal prophylaxis should be held during administration of these other systemic antifungal agents.
4.1.3 Concomitant Therapy Restrictions
4.1.3.1 Fluconazole
Some azoles, including fluconazole, have been associated with prolongation of the QT interval by electrocardiogram. Drugs known to prolong the QT interval should be used with caution or avoided with fluconazole. The administration of terfenadine with high dose fluconazole ( adult dose) and cisapride with any dose of fluconazole is contraindicated. A list of drugs that prolong the QT interval can be found at http://www.azcert.org.
Clinically or potentially significant drug interactions with fluconazole and the following agents have been observed: oral hypoglycemics (tolbutamide, glyburide, glipizide), coumarin-type anticoagulants (e.g., warfarin), phenytoin, cyclosporine, rifampin, theophylline, rifabutin, tacrolimus, short-acting benzodiazepines (more pronounced with oral fluconazole), and oral contraceptives. Since rifampin enhances the metabolism of concurrently administered fluconazole and the dose of fluconazole may need to be increased, the use of rifampin in this study should be avoided. Careful monitoring is required when fluconazole is administered with the other drugs.
Coadministration of oral fluconazole with combination contraceptives has resulted in an overall mean increase in ethinyl estradiol and levonorgestrel levels. However, in some patients, levels of ethinyl estradiol and levonorgestrel decreased by up to and , respectively. While there is evidence that fluconazole can inhibit the metabolism of ethinyl estradiol and levonorgestrel, there is no evidence that fluconazole can induce the metabolism of these drugs. The clinical significance of the above effects is currently undetermined and may simply be a product of inter-individual variation in metabolism.
Fluconazole inhibits several cytochrome P450 (CYP450) isoenzymes and may increase the serum level of drugs metabolized by CYP450 especially at high doses ( adult dose). For a list of drugs metabolized by the CYP450 system see http://medicine.iupui.edu/flockhart.
4.1.3.2 Caspofungin
Coadministration of caspofungin with certain inducers of drug clearance and/or mixed inducer/inhibitors (e.g., efavirenz, nevirapine, phenytoin, rifampin, dexamethasone, and carbamazepine) may result in clinically important reductions in plasma caspofungin concentrations. Cyclosporine increases caspofungin area under the concentration curve (AUC) which results in a transient elevation of ALT/SGPT and AST/SGOT. Therefore, the use of these interacting drugs should be avoided if possible.
Patients randomized to this regimen will start prophylaxis within 24-72 hours following completion of each systemic chemotherapy course. Continue prophylaxis until:
following the nadir.
OR
The next chemotherapy course.
OR
Patient meets any of the off protocol therapy criteria (Section 8.1).
If other systemic antifungal therapy is initiated for empiric therapy or treatment of suspected infection, then fluconazole prophylaxis should be held and fluconazole should resume when other systemic antifungal therapy is discontinued if this occurs prior to ANC recovery.
Administration of assigned fluconazole prophylaxis continues with subsequent courses of chemotherapy until the patient meets any off-protocol criteria including proven or probable IFI according to institutional diagnosis.
FLUCONAZOLE: by slow IV infusion over 1-2 hours* (or longer) OR by mouth.
Once daily.
Dose:
Age months to 17.99 years: day once daily (maximum dose: day)
Age years to 30 years: day once daily (maximum dose: day)
*For IV: The rate of infusion should not exceed hour
Oral fluconazole is available as , and 200 mg tablets and as an oral suspension at a concentration of 10 or .
Rounding: When tablets are used, round the dose to the closest 50 mg .
Round the suspension volume to the closest tenth of a mL . Round 0.05 mL up (e.g., round 3.15 mL to 3.2 mL ).
Oral fluconazole can be taken at any time during the day with or without food. It should be administered at approximately the same time each day. If vomiting occurs within 30 minutes of taking the dose, the dose may be repeated once. If a dose is missed, it should be taken immediately and only if there are at least 12 hours until the next scheduled dose.
SEE SECTION 5.0 FOR DOSE MODIFICATIONS FOR TOXICITIES. For COG Supportive Care Guidelines see https://members.childrensoncologygroup.org/prot/reference materials.asp
The therapy delivery map (TDM) for fluconazole prophylaxis is on the next page.
Following completion of prophylaxis in each course of chemotherapy, prophylaxis will restart at the end of the subsequent chemotherapy course as outlined above.
4.2.1. Fluconazole Treatment Arm.
Patients randomized to fluconazole arm.
Patient name or initials
DOB
Prophylaxis with fluconazole begins within 24-72 hours following completion of each systemic chemotherapy course. Extensive administration details are in Section 4.2. This TDM is on One (1) page.
DRUG
ROUTE
DOSAGE
DAYS
IMPORTANT NOTES
OBSERVATIONS
FLUCONAZOLE
Slow IV infusion over 1-2 hours* (or longer) OR by mouth.
months - 17.99 years: day (IV or enteral dose)
Maximum dose:
18-30 years: day (IV or enteral dose)
Maximum dose:
Once daily
Start within 24-72 hours following completion of each systemic chemotherapy course.
*For IV: The infusion rate should not exceed 200 mg /hour.
See Section 4.2 for oral drug administration.
a. CBC, diff, plts, creatinine, SGPT, SGOT, bilirubin
b. IFI Checklist (see Section 10.2)
Optional:
c. Galactomannan and beta-D glucan testing
d. SNP
OBTAIN OTHER STUDIES AS
REQUIRED FOR GOOD
PATIENT CARE
Enter Chemotherapy Course # Here_Ht_cm Wt_kg BSA_ m²
Date Due
Date Given
Day
FLUCONAZOLE mg
Studies
Comments (Include any held doses, or dose modifications)
Enter calculated dose above and actual dose administered below
mg
a, c
End Date:
Continue prophylaxis until criteria in Section 4.2 are met. Following completion of prophylaxis in each course of chemotherapy, prophylaxis will restart at the end of the subsequent chemotherapy course as outlined in Section 4.2.
Collect twice weekly. See Section 13 for details. It is suggested that specimens be obtained on Mondays & Thursdays; specimens may be obtained days from defined days as long as a minimum of 2 days separate each specimen collection. Obtain at end of Course 1, optimally when the patient has ANC and no circulating blasts. See Section 14 for details.
SEE SECTION 5.0 FOR DOSE MODIFICATIONS FOR TOXICITIES and the COG website posted materials for Supportive Care Guidelines https://members.childrensoncologygroup.org/prot/reference materials.asp
4.3 Administration Schedule- CASPOFUNGIN ARM
Patients randomized to this regimen will start prophylaxis within 24-72 hours following completion of each systemic chemotherapy course. Continue prophylaxis until:
following the nadir.
OR
The next chemotherapy course.
OR
Patient meets any of the off protocol therapy criteria (Section 8.1).
If other systemic antifungal therapy is initiated for empiric therapy or treatment of suspected infection, then caspofungin prophylaxis should be held and caspofungin should resume when other systemic antifungal therapy is discontinued if this occurs prior to ANC recovery.
Administration of assigned caspofungin prophylaxis continues with subsequent courses of chemotherapy until the patient meets any off-protocol criteria including proven or probable IFI according to institutional diagnosis.
CASPOFUNGIN: by slow IV infusion over no less than hour.
Loading dose (LD): day* - First day of therapy (Maximum dose: day).
Maintenance dose (MD): day* - Subsequent days (Maximum dose: day).
*Use the Mosteller Formula for BSA calculation.
SEE SECTION 5.0 FOR DOSE MODIFICATIONS AND TOXICITIES.
The therapy delivery map (TDM) for caspofungin prophylaxis for chemotherapy-induced neutropenia is on the next page.
Following completion of prophylaxis in each course of chemotherapy, prophylaxis will restart at the end of the subsequent chemotherapy course as outlined above.
4.3.1 Caspofungin Treatment Arm
Patients randomized to caspofungin arm.
□
DOB
Prophylaxis with caspofungin begins within 24-72 hours following completion of each systemic chemotherapy course. Extensive administration details are in Section 4.3. This TDM is on One (1) page.
DRUG
ROUTE
DOSAGE
DAYS
IMPORTANT NOTES
OBSERVATIONS
CASPOFUNGIN
IV over 1 hour
day day
1 2 (and subsequently)
Start within 24-72 hours following completion of each systemic chemotherapy course.
Maximum Loading dose:
Maximum Maintenance dose:
a. CBC, diff, plts, creatinine, SGPT, SGOT, bilirubin
b. IFI Checklist (see Section 10.2)
Optional:
c. Galactomannan and beta-D glucan testing
d. SNP
OBTAIN OTHER STUDIES AS REQUIRED FOR GOOD PATIENT CARE
Enter Chemotherapy Course # Here
Date Due
Date Given
Day
CASPOFUNGIN
Day 1: mg; Day 2 and Subsequently: mg
Studies
Comments (Include any held doses, or dose modifications)
Enter calculated dose above and actual dose administered below
1
LD:
2
MD: mg
□
End Date:
b,
Continue prophylaxis until the criteria in Section 4.3 are met. Following completion of prophylaxis in each course of chemotherapy, prophylaxis will restart at the end of the subsequent chemotherapy course as outlined in Section 4.3.
& twice weekly. See Section 13 for details. It is suggested that specimens be obtained on Mondays & Thursdays; specimens may be obtained days from defined days as long as a minimum of 2 days separate each specimen collection. Obtain at end of Course 1, optimally when the patient has ANC and no circulating blasts. See Section 14 for details.
SEE SECTION 5.0 FOR DOSE MODIFICATIONS FOR TOXICITIES and the COG website posted materials for Supportive Care Guidelines https://members.childrensoncologygroup.org/prot/reference materials.asp
5.0 DOSE MODIFICATIONS FOR TOXICITIES
5.1 Impaired Renal Function
When estimating renal function for adjusting drug doses, use the Schwartz formula for patients years of age and the Cockcroft and Gault equation for patients years of age.
Fluconazole:
Creatinine clearance
Percent of dose
Dose in mg/kg (max dose)
to 17.99 years:
years to 30 years:
dialysis
Hemodialysis
after each
dialysis
after each dialysis
after each dialysis
Note: When renal function improves to , the dose can be increased to the full dose.
Caspofungin:
Adjustment of the dose is not needed in the setting of impaired renal function. Caspofungin is not dialyzable and supplementation is not required following hemodialysis.
5.2 Impaired Liver Function
Fluconazole:
Fluconazole should be held in patients who develop signs and symptoms consistent with liver disease or elevations in hepatic function tests as defined by an ALT or AST ULN or serum bilirubin ULN.
Caspofungin:
For all patients:
Child - Pugh
score
Percent of dose
Dose in mg/kg (max dose)
Mild (5-6)
Loading dose: dose
Maintenance dose: dose
Moderate
Loading dose-100%
Maintenance dose-
Loading dose: dose
Maintenance dose: dose
Severe
Hold
Hold
To calculate the Child-Pugh Score:
Factor
1 Point
2 Points
3 Points
Total Bilirubin (mg/dL)
< 2.0
2.0-3.0
> 3.0
Albumin (g/dL)
> 3.5
2.8-3.5
< 2.8
INR
< 1.7
1.7-2.2
> 2.2
Ascites
No Ascites
Ascites, controlled
Ascites, poorly controlled
Encephalopathy
No Encephalopathy
Encephalopathy, controlled
Encephalopathy, poorly controlled
Caspofungin may be restarted or increased if liver function (and Child-Pugh score) improves.
6.0 DRUG INFORMATION
6.1 FLUCONAZOLE (Diflucan )
Source and Pharmacology:
Fluconazole is a triazole antifungal agent. It is structurally related to imidazole-derivative azole antifungal agents (e.g., clotrimazole, ketoconazole, miconazole) however, imidazoles have 2 nitrogens in the azole ring (imidazole ring) and fluconazole and other triazoles (e.g., itraconazole, terconazole) have 3 nitrogens in the ring (triazole ring). In addition, fluconazole contains a second triazole which makes it a bistriazole derivative and a halogenated phenyl ring. Replacement of the imidazole ring with a triazole ring apparently results in increased antifungal activity and an expanded antifungal spectrum of activity. Presence of the two triazole rings may contribute to fluconazole's resistance to first-pass metabolism and the drug's low lipophilicity and protein binding. Presence of a halogenated phenyl ring increases antifungal activity and contributes to the aqueous solubility which make fluconazole suitable for IV formulation.
Fluconazole is a highly selective inhibitor of the fungal cytochrome P-450 dependent lanosterol 14-alpha-demethylase. This enzyme converts lanosterol to ergosterol. The subsequent loss of normal sterols correlates with the accumulation of 14 alpha-methyl sterols in fungi and may be responsible for the fungistatic activity of fluconazole. Mammalian cell demethylation is much less sensitive to fluconazole inhibition.
Fluconazole is active against many fungi, including yeasts and dermatophytes. Fluconazole has been shown to be active against most strains of the following microorganisms both in vitro and in clinical infections: Candida ( ) albicans, glabrata (many strains are intermediately susceptible), parapsilosis, C tropicalis, and Cryptococcus neoformans. Candida krusei is considered to be resistant to fluconazole. Resistance to fluconazole may arise from a modification in the quality or quantity of the target enzyme (lanosterol 14- -demethylase), reduced access to the drug target by efflux of fluconazole out of the cell, or some combination of these mechanisms.
The pharmacokinetics of fluconazole are similar following IV or oral administration. In healthy adults receiving 50 - or doses of fluconazole given once daily by IV infusion over 30 minutes, serum concentrations of the drug 1 hour after dosing on the sixth or seventh day of therapy ranged from 2.142.81 or , respectively. In a multiple-dose study in children years of age, IV administration of , , or doses of fluconazole resulted in mean peak plasma concentrations of , or , respectively. Fluconazole is widely distributed into body tissues and fluids following oral or IV administration. In adult humans with normal renal function, concentrations of the drug in urine and skin may be 10 times higher than concurrent plasma concentrations. Concentrations in
saliva, sputum, nails, blister fluid, blister skin, and vaginal tissue are approximately equal to concurrent plasma concentrations. Fluconazole, unlike some azole-derivative antifungal agents (e.g., itraconazole, ketoconazole), distributes readily into the CSF following oral or IV administration. Another difference from other azole-derivative antifungals (e.g., itraconazole, ketoconazole, miconazole), is that fluconazole is only bound to plasma proteins while the other azole derivatives are highly protein bound.
The plasma elimination half-life of fluconazole in adults with normal renal function is approximately 30 hours (range: 20-50 hours). The mean plasma half-life of fluconazole in children 5 to 15 years of age after multiple IV doses is at the range of 15-18 hours. In healthy adults, fluconazole is eliminated mainly by renal excretion with approximately excreted in the urine as unchanged drug. Small amounts of the drug are excreted in feces. Metabolism accounts for only of total drug excreted. The renal clearance rate in adults is 0.27 to and in children age 5 to 15 years it is 0.4 to .
Some azoles, including fluconazole, have been associated with prolongation of the QT interval on the electrocardiogram. Fluconazole should be administered with caution to patients with this potentially proarrhythmic condition. Clinically or potentially significant drug interactions between fluconazole and the following agents/classes have been observed: oral hypoglycemics (tolbutamide, glyburide, glipizide), coumarin-type anticoagulants (e.g., warfarin), phenytoin, cyclosporine, rifampin, theophylline, terfenadine, cisapride, astemizole, rifabutin, tacrolimus, short-acting benzodiazepines (more pronounced with oral fluconazole). Coadministration of oral fluconazole with combination contraceptives has resulted in an overall mean increase in ethinyl estradiol and levonorgestrel levels. However, in some patients levels of ethinyl estradiol and levonorgestrel decreased by up to and , respectively. The clinical significance of the above effects is currently undetermined and may simply be a product of interindividual variation in metabolism.
Stevens-Johnson syndrome and toxic epidermal necrolysis, hypokalemia, hypercholesterolemia, hypertriglyceridemia, leucopenia including neutropenia and agranulocytosis, eosinophilia, thrombocytopenia , hepatitis, cholestasis, fulminant liver failure
Delayed: Any time later during therapy, excluding the above conditions
Alopecia with prolonged used
Unknown Frequency and Timing:
Pregnancy Category C. There are no adequate and well controlled studies in pregnant women. There have been reports of multiple congenital abnormalities in infants whose mothers were being treated for 3 or more months with high dose ( day of fluconazole. The relationship between
(L) Toxicity may also occur later.
Formulation and Stability:
Fluconazole injection is an iso-osmotic, sterile, nonpyrogenic solution of fluconazole in a sodium chloride or dextrose diluent. Each mL contains 2 mg of fluconazole and 9 mg of sodium chloride or 56 mg of dextrose. The pH ranges from 4.0 to 8.0 in the sodium chloride diluent and from 3.5 to 6.5 in the dextrose diluent. Injection volumes of 100 mL and 200 mL are packaged in glass or in polyvinylchloride (PVC) bags. Specific storage requirements may vary among manufacturers. In general, fluconazole injection in glass bottles or PVC bags should be stored between or between , respectively. Brief exposure to does not adversely affect the product in the PVC container. Fluconazole solution should be protected from freezing. The overwrap moisture barrier should not be removed from the PVC bags until ready for use. The solution should not be used if it is cloudy or precipitated.
Fluconazole is available as , or 200 mg tablets that may contain lactose. Fluconazole for oral suspension contains 350 mg or 1400 mg of fluconazole powder in bottles which may contain sucrose and sodium benzoate. The tablets and dry powder of fluconazole for oral suspension should be stored between .
CANADIAN SITES:
Fluconazole injection is only available as . Oral fluconazole is available as 50 mg , 100 mg 150 mg and 200 mg tablets. Fluconazole powder for oral suspension is only available as 350 mg of powder per bottle. Other product specifications are similar.
Guidelines for Administration: See Treatment and Dose Modification sections of the protocol.
Injection:
Fluconazole injection is provided as a solution in NS or that is ready to infuse without further dilution. The infusion may be prepared according to standard operating procedures of the institution. For example, the calculated dose volume in NS or may be is transferred to an evacuated PVC infusion bag or to an evacuated glass bottle. Since fluconazole solution contains no preservatives, and as with all parenteral drug products, aseptic technique must be used during the preparation of the dose. Institution guidelines should be followed for determining the expiration time of the infusion solution.
Oral:
To mix the oral suspension tap bottle until all the powder flows freely. To reconstitute, add 24 mL distilled water or Purified Water (USP) to the fluconazole 350 mg or 1400 mg powder in bottle and shake vigorously to suspend the powder. The concentration of the reconstituted suspension is for the 350 mg bottle and for the 1400 mg bottle with a total volume of 35 mL of suspension per bottle. The reconstituted suspension should be stored between and . Protect from freezing. Discard unused portion 2 weeks after reconstitution. Patients should be instructed to shake the oral suspension well before using. Oral fluconazole should be administered with or without food at approximately the same time each day and can be taken at any time during the day.
Supplier: Commercially available from various manufacturers. See package insert for further information.
6.2 CASPOFUNGIN (caspofungin acetate, Cancidas )
Source and Pharmacology:
Caspofungin acetate, a semisynthetic lipopeptide synthesized from a fermentation product of Glarea lozoyensis, is an echinocandin antifungal agent. It inhibits the synthesis of beta (1, 3)-D-glucan, an essential component of filamentous fungal cell wall that is not present in mammalian cells. Caspofungin has been shown to be active both in vitro and in clinical infections against most strains of the following organisms: Aspergillus (A) fumigatus, A flavus, A terreus, Candida (C) albicans, C glabrata, C guilliermondii, C krusei, C parapsilosis, C tropicalis. Following an intravenous infusion, the plasma concentration of caspofungin declines in a polyphasic manner. A short alpha-phase that occurs immediately post-infusion is followed by a beta-phase (half-life of 9 to 11 hours) and an additional, longer half-life phase, gamma-phase (half-life of hours). Caspofungin is extensively (about ) protein bound to albumin and is cleared mainly by distribution (rather than excretion or biotransformation). Caspofungin is slowly metabolized in the liver via hydrolysis and -acetylation. Following a single intravenous dose, of the parent drug and metabolites was excreted in feces and was excreted in the urine. After multiple doses of caspofungin day were given intravenously to adults, the total body clearance was . When a dose of day was given intravenously to children and adolescents, the total body clearance was in adolescents (12 to 17 years of age), in children 2 to 11 years and in children 3 to 23 months.
Caspofungin is not a substrate for P -glycoprotein and is a poor substrate for, and does not inhibit or induce, cytochrome P-450 isoenzymes in vitro. However, coadministration of caspofungin with certain inducers of drug clearance and/or mixed inducer/inhibitors (e.g., efavirenz, nevirapine, phenytoin, rifampin, dexamethasone, and carbamazepine) may result in clinically important reductions in plasma caspofungin concentrations. Cyclosporine increases caspofungin area under the curve (AUC) which results in a transient elevation of alanine transaminase (ALT) and aspartate transaminase (AST) and coadministration with tacrolimus may decrease tacrolimus AUC.
U.S. Food and Drug Administration's Pregnancy Category: Category C. It is not known if caspofungin crosses the placenta in humans. There are no adequate and well-controlled studies with the use of caspofungin in pregnant women.
In animal studies, caspofungin acetate has been shown to be embryotoxic. Abnormalities in rats, treated with caspofungin doses comparable to the human dose, included incomplete ossification of the skull and torso and increased incidence of cervical rib. In rabbits, incomplete ossifications of the talus/calcaneus were noted. In rats and rabbits caspofungin crossed the placenta and was evident in fetal plasma.
Formulation and Stability:
Caspofungin is available as a lyophilized white to off-white powder/cake as a single-use vial in two vial sizes ( 50 mg and 70 mg ). Each vials contains an intentional overfill. The 50 mg vials contain 54.6 mg and the 70 mg vial contains 75.6 mg . The 50 mg vials also contain 39 mg of sucrose and 26 mg of mannitol. The 70 mg vials also contain 54 mg of sucrose and 36 mg of mannitol. The pH is adjusted during manufacturing with glacial acetic acid and sodium hydroxide. The lyophilized powder vials should be stored refrigerated at to ( 36 to ).
Guidelines for Administration: See Treatment and Dose Modification sections of the protocol.
Preparation instructions in this monograph apply only to the Merck USA product as supplied for this study.
Prior to reconstitution, equilibrate the refrigerated vial to room temperature. Aseptically add 10.8 mL of Sodium Chloride Injection, Sterile Water for Injection, Bacteriostatic Water for Injection with methylparaben and propylparaben, or Bacteriostatic Water for Injection with benzyl alcohol to the
vial. Use diluents without benzyl alcohol for neonates and infants years of age or patients with hypersensitivity to benzyl alcohol.
The concentration of the reconstituted solution depends on the vial size and is listed in the table below:
CANCIDAS vial*
Total Drug Content (including overfill)
Reconstitution Volume to be added*
Resulting Concentration following Reconstitution**
50 mg
54.6 mg
10.8 mL
70 mg
75.6 mg
10.8 mL
*Preparation instructions apply only to the Merck USA product as provided in this study.
**Note different concentrations following reconstitution of the product in the vial.
The white to off-white cake will dissolve completely. Mix gently until a clear solution is obtained. Visually inspect the reconstituted solution for particulate matter or discoloration during reconstitution and prior to infusion. Do not use hazy, precipitated, or discolored solutions. The reconstituted solution may be stored for up to 1 hour at ( ). Since caspofungin vials are for single use only; the remaining solution should be discarded.
Dilute the appropriate volume of reconstituted caspofungin in or Sodium Chloride Injection or Lactated Ringers Injection. The final concentration should not exceed . The stability of the diluted solution for administration is 24 hours if stored at or 48 hours if stored refrigerated at 2 to ( 36 to ). Since the infusion solution contains no preservatives and as with all parenteral drug products, aseptic technique must be used during the preparation of the infusion bag. Institution guidelines should be followed to determine the expiration time of the infusion solution. The expiration time should not exceed 24 hours at and 48 hours refrigerated.
Caspofungin is administered by slow intravenous infusion over no less than 1 hour. Do not mix or coinfuse caspofungin with other medications, as there are no data available on the compatibility of caspofungin with other intravenous medications. DO NOT USE DILUENTS CONTAINING DEXTROSE since caspofungin is not stable in diluents containing dextrose. The infusion line should be flushed with sodium chloride before and after drug administration.
Supplier: Caspofungin will be supplied by the manufacturer Merck & Company, Inc., USA. The University of Pennsylvania School of Medicine will distribute the study medication to the study sites through their Investigational Drug Service Pharmacy. Drug ordering and drug destruction information can be found on the study website. Drug receiving and accountability records should be maintained and performed according to local institutional procedures.
If local regulations do not allow for dispensing of investigational drug supply for home use, commercial drug supply may be used for patients at home. All hospitalized patients must receive drug from investigational inventory.
7.0 EVALUATIONS/MATERIAL AND DATA TO BE ACCESSIONED
Timing of protocol therapy administration, response assessment studies, and surgical interventions are based on schedules derived from the experimental design or on established standards of care. Minor unavoidable departures (up to 72 hours) from protocol directed therapy and/or disease evaluations (and up to 1 week for surgery) for valid clinical, patient and family logistical, or facility, procedure and/or anesthesia scheduling issues are acceptable per COG administrative Policy 5.14 (except where explicitly prohibited within the protocol).
All baseline studies must be performed prior to starting protocol therapy unless otherwise indicated below.
7.1 Required and Optional Clinical, Laboratory and Disease Evaluations Obtain prior to start of phase unless otherwise indicated.
STUDIES TO BE OBTAINED
Baseline
Course
Subsequent Courses
End of ACCL0933 Therapy
REQUIRED
History
X
Physical Exam (Ht, Wt, BSA)
X
CBC, differential, platelets
X
X
X
X
Creatinine, SGPT, SGOT, bilirubin
X
X
X
X
IFI checklist
X*
X*
X*
OPTIONAL
Sample for SNP Genotyping
GM, BG Assays
2x weekly
2x weekly
# Course 1 of fluconazole or caspofungin follows Course 1 of AML therapy. Subsequent Courses refers to protocol-directed antifungal prophylaxis, not AML therapy.
Submit relevant IFI checklist documents via the Document Imaging System: (626) 447-2204 at the end of each course of protocol therapy. See Section 10.2 for further details.
% Obtain at end of Course 1, optimally when the patient has ANC and no circulating blasts. Collect specimens twice weekly during the period of neutropenia (until ANC ). See Section 13.1 for specimen collection details. It is suggested that specimens be obtained on Mondays and Thursdays but other days are acceptable if more convenient. A minimum of 2 days should separate each specimen collection. All specimens must be collected in the specimen vials provided by MiraVista Laboratories in the shipped lab collection kits. Alternative specimen vials should never be used as they may contribute to false results.
This table only includes evaluations necessary to answer the primary and secondary aims. Obtain other studies as indicated for good clinical care.
7.2 Optional Studies
7.2.1 Galactomannan and ( ) Beta-D Glucan Assays
Two antifungal antigen assays (Platelia Aspergillus EIA and Fungitell Assay) will be performed during the period of neutropenia in order to identify IA only and all IFI respectively. 6 mL of peripheral blood will be collected in a gold top serum-separator tube (provided by MiraVista) twice weekly. See Section 13 for sample collection, processing and shipping details. For each period of neutropenia, documentation of exposure or lack of exposure to each of the following will be performed: amoxicillin-clavulanate, piperacillin-tazobactam, and intravenous immunoglobulin. Documentation of infection with Pneumocystis jiroveci, Penicillium spp., Histoplasma capsulatum, Geotrichum spp., or Neosartoria spp. will occur through microbiology or pathology reporting and through routine adverse event reporting. See Section 11 for sample collection and shipping details.
7.2.2 SNP Analysis
Genotyping will be conducted in order to determine genes mediating immune function. Patients enrolled on AAML1031 will require no additional sample collection to participate. For all other patients, 5 mL of peripheral blood will be collected in a purple top tube at the end of Course I, optimally when the patient has an ANC (and with no circulating blasts). See Section 14 for sample collection and shipping details.
8.0 CRITERIA FOR REMOVAL FROM PROTOCOL THERAPY AND OFF STUDY CRITERIA
8.1 Criteria for Removal from Protocol Therapy
a) Development of proven or probable IFI including IA according to institutional diagnosis.
b) Patients who begin conditioning for HSCT.
c) Begin a new chemotherapy regimen for AML that is refractory to, or relapsed with current AML chemotherapy.
d) Refusal of further protocol therapy by patient/parent/guardian.
e) Recovery from neutropenia following completion of the final planned AML chemotherapy course .
f) Physician determines it is in patient's best interest.
Patients who are off protocol therapy are to be followed until they meet the criteria for Off Study below. Follow-up data will be required unless consent was withdrawn. A patient that is placed on empiric fungal therapy for prolonged fever and neutropenia should NOT be removed from protocol therapy for subsequent AML chemotherapy courses unless one of the off protocol therapy criteria is met.
8.2 Off Study Criteria
a) Death.
b) Lost to follow-up.
c) Withdrawal of consent for any further data submission.
d) Second anniversary of study entry.
8.3 Discontinuation from IFI Observation Criteria
Patients who are taken off protocol therapy (but are not off study) must be followed for all infection endpoints until they meet the Discontinuation from IFI Observation Criteria (below) or until they meet the Off Study Criteria (See Section 8.2).
a) Begin conditioning for HSCT.
b) Begin a new chemotherapy regimen for AML that is refractory to, or relapsed with current AML chemotherapy.
c) Two weeks after recovery from neutropenia following completion of the final planned AML chemotherapy course.
9.0 STATISTICAL CONSIDERATIONS
9.1 Statistical Design
This is a randomized open-label trial to determine if prophylaxis with caspofungin during periods of neutropenia following chemotherapy for AML is associated with a lower incidence of proven or probable IFI compared with fluconazole. Eligible AML patients at ages 3 months to 30 years will be randomized to receive daily prophylaxis with either caspofungin or fluconazole. Randomization will be stratified into 2 groups: 1) de novo AML vs. 2) all other patients.
9.2 Patient Accrual and Expected Duration of Trial
Eligible subjects will have de novo, relapsed, or secondary AML, or any diagnosis being treated with institutional standard AML therapy (for example myelodysplastic syndrome, bone marrow blasts > 5% or biphenotypia). This protocol does not require concurrent enrollment on a COG therapeutic protocol. Patients treated per the upcoming de novo AML protocol, AAML1031 but not enrolled (for example, due to failure to meet AAML1031 eligibility criteria, refusal or other reasons) may enroll on ACCL0933. The de novo AML therapeutic protocol, AAML0531, accrued over 300 patients per year and the subsequent de novo AML protocol, AAML1031, is projected to accrue about 290 patients per year. The potential patient pool for ACCL0933 will be larger than AAML1031, and therefore, the accrual rate for this study is expected to be about 150 patients per year. Taking into account the initial delay in opening the study at institutions, the expected total accrual duration for 550 eligible patients is about 4 years. The maximum accrual, including ineligible enrollments, is 575 patients.
9.3 Statistical Analysis Methods
9.3.1 Study Endpoints
Primary endpoint
The primary endpoint is the development of proven or probable IFI defined according to criteria developed by the European Organization for Research and Treatment of Cancer/Mycoses Study Group (EORTC/MSG) (from which time to IFI will be computed).
Secondary Endpoints
Endpoints for secondary objectives include: the development of proven or probable IA defined according to criteria developed by the EORTC/MSG (from which time to IA will be computed), death due to any cause (from which time to death will be computed), the need for empiric antifungal therapy defined as the institution of antifungal therapy while a study subject is receiving prophylaxis (from which the days of empirical antifungal therapy will be computed), results from GM and beta-D glucan assays for the diagnosis of IFI or IA alone, and results of the genotyping assays for SNP analysis.
An exploratory endpoint will be the development of proven, probable or possible IFI.
9.3.2 Central Committee Review
In order to ensure consistent and accurate application of the EORTC/MSG guidelines across all study patients, a Central Review Committee including Pediatric Oncologists and Pediatric Infectious Disease Specialists will be assembled. Through consensus meetings, committee members will review all data pertinent to the EORTC/MSG guidelines and determine whether a patient sustained a possible, probable or proven IFI or IA infection during the study period. The following data for each study patient will be collected and available at the time of the review: pathology reports, all CT scan and MRI reports, fungal Gram stain and microbiology culture results, non-culture mycology testing results (i.e., Histoplasma urine antigens, cryptococcal CSF and serum antigens), ophthalmology exams, bronchoscopy reports, and dosing and duration of steroid exposures.
All reviewers will be blinded to the patient's antifungal exposures in order to limit any bias in determining the primary and secondary endpoints.
9.3.3 Sample size with power justification
A total of approximately 550 eligible patients will be randomized to the 2 arms (at least 275 patients on each arm). Patients will be followed for infection outcome data until criteria in Section 8.3 has been met unless the patient is off study per Section 8.2 prior to meeting criteria in 8.3.
Since the current AAML1031 proposal plans 4 courses of chemotherapy with about 1 month duration for each course, it implies that likely many study participants will be followed for IFI for about 5 months. The power calculation assumes an IFI incidence in the fluconazole group of and an IFI incidence in the caspofungin treatment groups of at 5 months. The hazard ratio is 0.24 . We assume up to of patients may have early termination of follow up on IFI due to change in AML therapy such as refractory disease, relapse, or death. It is estimated that up to of patients treated on or per AAML1031 may go to SCT prior to finishing all 4 courses. Therefore, altogether up to patients may not be followed until the end of 5 months for IFI. With at least 275 patients on each arm, a planned 5 -month follow up on each patient and up to patients being censored by 5 months, we have about power to detect the expected difference in time-to-IFI curves between the 2 arms ( vs. at 5 months) in a log rank test with 2 -sided alpha level of 0.05 . In the calculation, both failure and censoring are assumed to follow an exponential distribution during the 5 months. The majority of the censoring events prior to 5 months are expected to be due to SCT which likely occur later in the 5 months, so the exponential censoring distribution might not be a very good approximation but should be conservative in power consideration.
The assumed baseline incidence of IFI of at 5 months is based on data reported in previous studies. CCG protocol 2961 found a incidence of IFI. The rate of microbiologically documented sterile site fungal infections documented on AAML0531 is as of April 2010; not all of these would meet MSG/EORTC criteria as proven/probable IFIs. In the power calculation, the onset of IFI in both groups over the 5 -month period is assumed to follow an exponential distribution and is and for fluconazole and caspofungin at 5 months respectively. Under such exponential models, the incidence of over 5 months is approximately even, about per month for fluconazole and per month for caspofungin.
In this setting, we have a potential competing risk issue but its impact on estimating the risk for IFI should be minimal. We expect that majority of the censoring for IFI prior to the study completion are due to SCT or relapsed/refractory disease; the occurrence of such events are likely independent of the risk for IFI should the patient continue on the AML therapy, and can be considered true censoring events in the power consideration above. On the other hand, death prior to any other event constitutes a competing risk for IFI, but we expect such deaths to be rare and will not likely exceed during the first 5 months; the impact that it has on estimating the risk of IFI by treating it as censored is minimal. Recently there have been some developments on sample size considerations under competing risk setting for either the
proportional cause-specific hazard model or proportional sub-distribution hazard model. However since the cumulative incidence of IFI under competing risk setting also involves the cause specific hazard of the competing risk, the interpretation of some of the planning parameters in these settings can be complicated and additional assumptions about the competing risk need to be made; it is also not yet well understood which model is better in different real settings. Given the fact that the true competing risk here is rare, we still use standard survival analyses for sample size considerations, but will perform competing risk analyses on the study data to ensure that it does not change the results of the comparison.
9.3.4 Analysis Plans
Descriptive Analyses
Standard descriptive statistics will be used to describe subjects' baseline characteristics and study outcome measures overall and within each treatment group. Summary statistics such as means, standard deviations, medians, and ranges will be produced for all measured variables. The balance of baseline measures across the treatment groups will be examined using appropriate two-sample tests.
Analysis for Primary Objective and Secondary Clinical Objectives
The primary analysis will be based on the principle of intention to treat (i.e., by the treatment assignment of patients at randomization, regardless of subsequent compliance with the assigned treatment). Most of the events that take patients off IFI follow up prematurely such as going to SCT, relapse/refractory disease, may be considered independent from the risk for IFI; therefore they may be considered as true censoring events. Death before any such censoring events is a competing risk for IFI; however since the chance of that happening will be rare, expected to be no more than , the effect of competing risk by death as the first event should be minimal. Therefore, we will focus on standard survival analyses but will also perform competing risk analyses to check if the results change after we consider death as a competing risk. In standard survival analyses, patients who go off IFI follow up before developing IFI for any reason will be treated as being censored. We will use Kaplan-Meier analyses to evaluate time to any IFI and log rank test to assess if there is any benefit associated with caspofungin compared to fluconazole. For competing risk analyses, nonparametric estimate of the cumulative incidence function for IFI will then be calculated by treating death (if first event) or possibly death plus other events as competing risk for IFI; Gray's test will be used to compare the cumulative incidence function between the 2 arms.
Similar standard survival analyses and competing risk analyses will be performed for secondary objectives 1-3 and the exploratory endpoint. For the secondary objective of time to development of invasive aspergillosis (IA), other IFI will also be considered a competing risk variable for IA in the competing risk analysis. For time to death (by any cause), only standard survival analyses will be performed. The total days of empiric antifungal therapy will also be compared between the 2 arms using t-test or Wilcoxon rank sum test.
Analysis of GM and beta-D Glucan Assays
Sensitivity, specificity, positive predictive value, and negative predictive value of the GM assay and betaD glucan assay will be determined using standard formulas and EORTC/MSG criteria as the gold standard. Please see Section 13.8 for additional statistical considerations for this secondary aim.
SNP Analysis in Genes Involved in Immunity
We will perform haplotype analysis using previously established methods for unrelated subjects. To deal with possible false positive or negative results, we will perform the following. First, in order to handle the concern of multiple testing, we will adjust the value required for statistical significance by the false discovery rate, which is an approach to multiple testing that is a compromise between unadjusted tests of significance and more traditional, but too conservative Bonferonni adjustment. Second, to handle the potential for population stratification, all analyses will be performed with and without adjustment by ethnicity. We will use Kaplan-Meier analyses to evaluate time to any IFI, and determine
the impact of candidate gene SNPs using the log rank test. For the exploratory analysis on the relationship between IFI and the identified SNPs in the candidate genes, study participants will be grouped based on the genotype of specific . If the primary analysis suggests no difference in IFI between caspofungin and fluconazole, standard log rank analysis will be used to compare the time to IFI between patient groups defined by the ; stratified log rank test adjusting for treatment arm will be considered if the data suggest a treatment difference on IFI between caspofungin and fluconazole.
In developing a clinical prediction model for IFI, the outcome is time to IFI and the predictors can be demographic factors, clinical factors, co-morbid conditions, and SNPs. Standard survival analysis such as Cox model (or competing risk analyses modeling the cause-specific hazard or cumulative incidence function, if needed) will be used to build predictive models. Unlike an explanatory model, inclusion of variables into the predictive model will depend only on its ability to improve the prediction of the outcome and does not necessarily have to be based on biologic plausibility (although plausibility could make a prediction rule more accessible to clinicians). On the other hand, a clinically useful predictive model also needs to be practical in that the variables must be available in most clinical settings. We will take into account these factors in developing the predictive models, and internal cross-validation techniques will be considered in assessing the models.
9.3.5 Interim Monitoring
Study data will be reviewed by DSMC twice a year during the first 2 years of study activation, and once a year thereafter upon their approval if the study goes smoothly. We plan two formal interim efficacy analyses comparing treatment outcomes between the 2 arms, after approximately one third and two thirds of the patients have completed study treatment and IFI observation. The endpoints for the interim analyses include time to the following individual event: IFI, invasive aspergillosis, death. Log rank test will be the primary method for these interim analyses; monitoring boundary for the primary endpoint on IFI will be based on Lan-Demet's method with spending function t. Competing risk analyses such as estimating the cumulative incidence of the event and Gray's test for IFI or IA will be performed as well to check that corresponding competing risk analyses do not suggest a different conclusion than the standard survival analyses.
Informal interim safety analyses will also be performed at each DSMC review on the observed adverse events between the 2 arms. This analysis will include all patients who receive at least one dose of study medication. The proportion of patients experiencing any grade 4 or higher non-hematological adverse event will be compared between the 2 groups using chi-square tests. For this monitoring, each test will be at two-sided level of 0.05 without adjustment for multiple testing, to ensure us being alerted by any potential difference in adverse events between the 2 arms. If a significant difference between the 2 arms is found ( ), the study committee will examine the adverse event profiles for safety considerations and decide if any action needs to be taken.
9.4 Gender and Minority Accrual Estimates
The gender and minority distribution of the study population is expected to be:
Accrual Targets
Ethnic Category
Sex/Gender
Females
Males
Total
Hispanic or Latino
58
52
110
Not Hispanic or Latino
226
239
465
Ethnic Category: Total of all subjects
284
291
*575
Racial Category
American Indian or Alaskan Native
2
1
3
Asian
17
14
31
Black or African American
39
34
73
Native Hawaiian or other Pacific Islander
0
1
1
White
226
241
467
Racial Category: Total of all subjects
284
291
*575
These totals must agree.
This distribution was derived from AAML0531 and AAML00P2.
10.0 EVALUATION CRITERIA
10.1 Common Terminology Criteria for Adverse Events (CTCAE)
This study will utilize version 4 of the CTCAE of the National Cancer Institute (NCI) for toxicity and performance reporting. A copy of the CTCAE version 4 can be downloaded from the NCI website at: http://ctep.cancer.gov/protocolDevelopment/electronic_applications/ctc.htm. Additionally, toxicities are to be reported on the appropriate case report forms.
10.2 IFI Checklist and Central Review
Institutions will be provided with case report forms to complete which will help to identify whether patients had IFI (IFI checklist). Biopsy and imaging reports are requested rather than report interpretation in order to minimize the work load for sites. An independent data review committee including infectious disease and oncology experts who are unaware of treatment assignments will review and classify all cases of proven/probable IFI by EORTC/MSG.
The following materials in the IFI checklist will be submitted (via the Document Imaging System:
(626) 447-2204) at the end of each course of protocol therapy, only if they were performed to investigate an IFI according to local physician discretion:
Pathology reports (including autopsy reports),
CT scan and MRI reports,
Fungal Gram stain and microbiology culture results (including both positive and negative results),
Ophthalmology exams (even if evidence of fungi not seen), and
Bronchoscopy reports (even if evidence of fungi not seen).
In addition, dosing and duration of steroid exposure will be collected and entered via eRDE. All reviewers will be blinded to the patient's antifungal exposures in order to limit any bias in determining the primary and secondary endpoints.
11.0 ADVERSE EVENT REPORTING REQUIREMENTS
11.1 Purpose
Adverse event data collection and reporting, which are required as part of every clinical trial, are done to ensure the safety of patients enrolled in the studies as well as those who will enroll in future studies using similar agents.
11.2 Determination of Reporting Requirements
Reporting requirements may include the following considerations: 1) the characteristics of the adverse event including the grade (severity); 2) the relationship to the study therapy (attribution); and 3) the prior experience (expectedness) of the adverse event.
Commercial agents are those agents not provided under an IND but obtained instead from a commercial source. In some cases an agent obtained commercially may be used for indications not included in the package label. In addition, NCI may on some occasions distribute commercial supplies for a trial. Even in these cases, the agent is still considered to be a commercial agent and the procedures described below should be followed.
Determine the prior experience Expected events are those that have been previously identified as resulting from administration of the agent. An adverse event is considered unexpected, for reporting purposes only, when either the type of event or the severity of the event is not listed in:
the current known toxicities for each commercial agent as provided in the Drug Information for Commercial Agents Used by the Children's Oncology Group posted on the COG website; or
the drug package insert.
Secondary Malignancy
A secondary malignancy is a cancer caused by treatment for a previous malignancy (eg, treatment with investigational agent/intervention, radiation or chemotherapy). A metastasis of the initial neoplasm is not considered a secondary malignancy.
All secondary malignancies that occur following treatment need to be reported via CTEP-AERS. Three options are available to describe the event:
Leukemia secondary to oncology chemotherapy
Myelodysplastic syndrome
Treatment related secondary malignancy
11.3 Reporting of Adverse Events for Commercial Agents - via CTEP-AERS
Commercial reporting requirements are provided in Table B. The commercial agent(s) used in this study are listed in the front of this protocol immediately following the Study Committee roster.
COG requires the CTEP-AERS report to be submitted within 7 calendar days of learning of the event.
Use the NCI protocol number and the protocol-specific patient ID provided during trial registration on all reports.
CTCAE term (AE description) and grade: The descriptions and grading scales found in the NCI Common Terminology Criteria for Adverse Events (CTCAE) version 4 will be utilized for AE reporting and are located on the CTEP website at: http://ctep.cancer.gov/protocolDevelopment/electronic_applications/ctc.htm. All appropriate treatment areas should have access to a copy of the CTCAE.
Table B
Reporting requirements for adverse events experienced by patients on study who have NOT received any doses of an investigational agent on this study.
CTEP-AERS Reporting Requirements for Adverse Events That Occur During Therapy With a Commercial Agent or Within 30 Days
Attribution
Grade 4
Grade 5
Unexpected
Expected
Unrelated or Unlikely
CTEP-AERS
Possible, Probable, Definite
CTEP-AERS
CTEP-AERS
This includes all deaths within 30 days of the last dose of treatment with a commercial agent, regardless of attribution. Any death that occurs more than 30 days after the last dose of treatment with a commercial agent which can be attributed (possibly, probably, or definitely) to the agent and is not due to cancer recurrence must be reported via CTEP-AERS
11.4 Routine Adverse Event Reporting
Note: The guidelines below are for routine reporting of study specific adverse events on the COG case report forms and do not affect the requirements for CTEP-AERS reporting.
The NCI defines both routine and expedited AE reporting. Routine reporting is accomplished via the Adverse Event (AE) Case Report Form (CRF) within the study database. For this study, routine reporting will include all toxicities reported via CTEP-AERS and all Grade 4 and higher non-hematological Adverse Events.
12.0 RECORDS AND REPORTING
See the Case Report Forms posted on the COG web site with each protocol under "Data Collection/Specimens". A submission schedule is included.
12.1 CDUS
This study will be monitored by the Clinical Data Update System (CDUS). Cumulative CDUS data will be submitted quarterly to CTEP by electronic means. Reports are due January 31, April 30, July 31 and October 31. This is not a responsibility of institutions participating in this trial.
13.0 PROSPECTIVE EVALUATION OF GALACTOMANNAN AND BETA-D GLUCAN ASSAYS AS DIAGNOSTIC TOOLS FOR INVASIVE FUNGAL INFECTION IN CHILDREN WITH ACUTE MYELOID LEUKEMIA RECEIVING FUNGAL PROPHYLAXIS.
13.1 Sample Collection and Testing Procedures (These studies are optional)
13.1.1 Sample submission
At the time of enrollment, if a new patient has consented to the optional galactomannan and beta-D glucan study, a sample collection kit will be automatically express delivered to the treating institution. If the kit is not received within 48 hours of enrollment, please contact Patti Connolly at MiraVista (317-856 as soon as possible to prevent any further delays. The kit contains special vials that are mandatory for specimen collection. Alternative specimen vials should never be used as they may contribute to false results.
13.1.2 Sample Collection
Whole blood samples will be collected twice weekly during the period of neutropenia (until ANC ). It is suggested that specimens be obtained on Mondays and Thursdays but other days are acceptable if more convenient. A minimum of 2 days should separate each specimen collection.
In order to perform both assays on a single specimen (Platelia Aspergillus EIA and Fungitell beta-D glucan assay), collect 5 mL of whole blood in a gold top serum-separator tube (provided by MiraVista) and label with the site number, COG ID number, and date (labels will be provided with the sample shipping kit). Although the above volume of blood testing will likely represent a small fraction of the blood testing performed during the period of 1 week, it may result in an important increase in certain patients (i.e., smaller children or anemic children). Therefore, we have set the following maximum limits per kilogram for blood draws related to this ancillary study: 3 mL of blood body weight in an 8 week period.
13.1.3 Specimen processing
Each specimen should be processed as follows prior to shipping:
Allow the blood to clot for minutes at room temperature.
Centrifuge the specimen for 15 minutes at .
Remove the serum from the clot and place it into the provided polypropylene storage tube and label the tube.
A total minimum volume of 2 mL of serum is required to run the Platelia Aspergillus EIA and Fungitell beta-D glucan assay.
13.1.4 Storing specimens
Specimens should be frozen at the day of collection after following the above processing steps.
Specimens can be stored at until shipment. Specimens stored at may be stored indefinitely.
13.1.5 Shipping of specimens:
Each center will use shipping kits provided by MiraVista Diagnostics. These kits contain Styrofoam lined boxes, sealing tape, labels, and a cold pack. The boxes are designed to hold 10 frozen serum specimens. In order to optimize efficiency, a box should not be sent until 10 specimens have been collected.
Requisitions:
Complete an ACCL0933 GM & BG Requisition Form for each specimen sent for testing. All areas of the requisition form must be completed.
Packaging:
Assure all specimen labels and packaging labels are correct and legible. Please use the labels provided in the kits as they are designed to withstand specimen freezing and thawing without disruption of the written patient identification information. A Sharpie marker is most effective for writing on these labels.
Place the labeled vials containing the patient serum into a biohazard plastic bag along with absorbent material such as gauze or paper towel and seal. Use the biohazard plastic bags provided in the kit.
Ship specimens in the boxes provided along with the cold pack that should be frozen.
Open the box and remove the Styrofoam liner lid and the sealing tape.
Place the frozen cold pack into the liner. The frozen cold pack will ensure specimen integrity during overnight shipment.
Place the biohazard plastic bag containing the requisition forms and specimens directly on top of the frozen cold pack.
Replace the Styrofoam liner lid.
Complete an ACCL0933 GM & BG Requisition Form for each specimen and place them on top of the liner before sealing the box.
Wet the sealing tape provided in the kit and seal the cardboard box.
If the specimen tube labels and requisition forms do not match when received at MiraVista Diagnostics, a call will be made to the study site on the day of receipt.
Shipping Instructions:
Ship packages to the following address:
MiraVista Diagnostics
4705 Decatur Blvd.
Indianapolis, IN 46241
317-856-2681
Use the FedEx website (www.fedex.com) to learn the current guidelines for the shipping of human body fluids and generating shipping labels.
Generate a label via the FedEx website and schedule a pick up (use the MiraVista FedEx account provided).
Affix the FedEx label to the top of the box.
Ship all packages Priority Overnight via FedEx to arrive at MiraVista Diagnostics by 10:30 AM the next morning.
Do not ship on a Friday, Saturday, or the day before a holiday. MiraVista is closed each weekend and on holidays.
13.1.6 Testing of specimens:
Testing of serum specimens for this study will be performed in batches.
a. Negative results are final.
b. Positive results are retested on the next work day for confirmation.
Testing will not occur under the following conditions:
a. The specimen has been stored under unacceptable storage times and/or temperatures.
b. The specimen has been shipped under unacceptable time and/or temperature conditions.
c. The specimen volume is less than needed to complete the testing process.
d. The specimen cannot be pipetted due to viscosity.
e. The specimen is hemolyzed or icteric for Fungitell .
f. The specimen is of a type other than serum separated off the clot.
Platelia Aspergillus EIA results are reported as a GM index.
Fungitell beta-D glucan assay results are reported as .
13.1.7 MiraVista Contact Information
Technical Assistance: Patti Connolly 317-856-2681 x451
Medical Director: Joseph Wheat, M.D. 317-856-2681 x452
13.1.8 Galactomannan and Beta-D glucan Assays
Testing will be performed by technicians blinded to each patient's clinical information. Test results will not be made available to treating physicians since the utility of these tests is not yet established in children and because we will not be conducting testing in real time. Thus, results will not be utilized for clinical decision-making.
To our knowledge BG testing is not routinely performed at many pediatric centers but may be performed at some of the COG sites while GM testing is currently performed at a number of pediatric centers. Regardless of the number of institutions offering such testing options, we anticipate that such testing will be ordered by a subset of treating physicians. The local BG and GM results will not be included in our final analysis of the 2 biomarker assays' operating characteristics. However, these results may effect a change from fungal prophylaxis to preemptive or empiric therapy and may encourage or discourage more comprehensive efforts to diagnose a proven or probable IFI in any given patient. This in turn may falsely influence our evaluation of the 2 biomarker assays' operating characteristics. For each patient we will identify whether local BG or GM testing has been performed and, via a sensitivity analysis, explore whether such a practice influences the operating characteristics. The plans for this sensitivity analysis are described in more detail in Section 13.8.4 below.
The Platelia Aspergillus EIA study is reported as a GM index. We will use the FDA-approved threshold of GM index on a single test sample as our criteria for a positive test result. The Fungitell Assay is reported in pg per mL of patient's serum. The manufacturer recommendation for a single positive Fungitell assay result of will be used to define a positive test.
13.2 Background
13.2.1 Changing approach to antifungal therapy in pediatric AML patients
Various strategies for starting antifungal therapy in patients with cancer exist and include :
Prophylaxis: Initiation of antifungal therapy in asymptomatic patients without any evidence of IFI, during periods of high risk such as during prolonged neutropenia resulting from chemotherapy or bone marrow transplant.
Empirical antifungal therapy: Initiation or modification of antifungal therapy after persistence of fever in the setting of neutropenia and broad-spectrum antibiotics.
Preemptive therapy: Use of radiographic and/or specific biomarkers to identify and treat suspected IFI prior to overt clinical presentation.
Therapy for proven, probable or presumed IFI: Therapy initiated for the treatment of proven or probable IFI based on EORTC/MSG criteria or based on clinical presumption of IFI.
The significant morbidity and mortality associated with IFI among patients with AML has led many clinicians to adopt a strategy that includes antifungal prophylaxis during periods of neutropenia. Retrospective evaluation of neutropenic children receiving fungal prophylaxis with fluconazole or micafungin suggested a reduction in the risk for IFI. The ideal antifungal agent for such prophylaxis in children is not known and will be addressed in the primary aim of this study. Regardless of the specific antifungal agent, it is likely that prophylaxis will be successful and be integrated as the standard of care for all future pediatric AML therapy. Despite a reduction in IFI, prophylaxis will not eliminate all such infections. In patients with breakthrough infections on prophylactic therapy, early suspicion for IFI and modification of antifungal therapy will still be paramount to improving patient outcomes.
Unfortunately, the current approach for risk stratification of IFI (persistence of fever for days on broad spectrum antibiotics) may be less than ideal in populations at high risk for IFI. The clinical presentation at the start of an IFI can range from completely asymptomatic, to fever without localizing signs or symptoms, to clinical sepsis. This is illustrated by a randomized trial of empiric caspofungin vs. liposomal amphotericin B. Patients were excluded from this study if they had a current documented IFI. Despite this, 4.9% of subjects were ultimately identified as having proven or probable IFI at baseline prior to initiating the antifungal treatment. Therefore, relying on traditional methods to guide empiric antifungal modifications would result in over-treating some patients with low likelihood of IFI and a failure to modify therapy in other patients that have an underlying IFI. A preemptive therapeutic approach that utilizes screening diagnostic studies to identify patients likely to have an IFI at the earliest possible point may be more rational and successful.
13.2.2 Traditional diagnostic studies to identify patients with suspected IFI
Traditional diagnostic modalities for IFI are limited to radiologic imaging and blood or tissue culture techniques. Radiologic studies may show visceral involvement but an invasive biopsy procedure is necessary to differentiate between a fungal or non-fungal infectious process. Although blood cultures may be used to isolate Candida spp. during candidemia, they are not helpful in the setting of invasive candidiasis without fungemia. Furthermore, traditional blood cultures are not typically successful at isolating mold infections such as Aspergillus. Cultures of tissue specimens can be definitive but require invasive techniques for sample procurement.
13.2.3 Galactomannan and Beta-D Glucan Assays
Alternative non-invasive approaches involve serial evaluation of a patient's serum for the presence of galactomannan (GM) or beta-D glucan (BG). The former is present in Aspergillus spp. while the latter is present in a vast majority of pathogenic fungi. Two validated FDA approved antigen detection assays, The Platelia Aspergillus EIA and the Fungitell Assay, currently exist for the detection of GM and BG, respectively.
13.2.3.1 The Platelia Aspergillus EIA and Fungitell Assay in Adults
The Platelia Aspergillus EIA is a commercially available kit from Bio-Rad Laboratories that utilizes an EB-A2 monoclonal antibody and sandwich technique for detection of GM. In 2003, the assay received FDA approval for use in adults after it was prospectively validated in a cohort of immunosuppressed patients. This cohort included patients aged 16 years or older with various leukemias, lymphomas or those undergoing stem cell transplants. Twice a week testing was performed in 362 separate hospitalizations. Criteria for proven or probable invasive aspergillosis (IA) developed by the EORTC/MSG were used as the gold standard. This testing strategy resulted in sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV) for detection of IA. Detection of GM preceded the time of definitive IA diagnosis in of the proven IA cases by a median of 17 days. Two separate meta-analyses have since been performed which support the usefulness of GM screening in adults.
The Fungitell Assay (formerly Glucatell) is a commercially available kit from the Associates of Cape Cod, Inc. for the identification of BG in the serum of patients with IFI. This assay received FDA approval in May of 2004 to assist in the diagnosis of IFI. The operating characteristics of the assay have been elucidated in multiple adult cohorts. The first included adult patients with newly diagnosed AML or myelodysplastic syndrome undergoing initial Induction chemotherapy and receiving fungal prophylaxis with either caspofungin or itraconazole. The Fungitell Assay was performed in 283 patients twice a week for the duration of neutropenia resulting in sensitivity, specificity, PPV and NPV for diagnosing proven or probable IFI of , and , respectively. More importantly, a positive Fungitell Assay result was identified at a median of 10 days prior to the clinical diagnosis of IFI in this cohort.
The second study evaluated 95 adult patients with fever and neutropenia down to 16 years of age. Thirtyeight patients with proven, probable or possible IFI were identified. The resultant sensitivity, specificity, PPV and NPV were , and respectively. The specificity reported was reduced as compared to results from the prior publication as they included possible as well as probable and proven cases of IFI. Positive Fungitell Assay results preceded clinical diagnosis of IFI by a median of 5 days.
13.2.3.2 The Platelia Aspergillus EIA and Fungitell Assay in Children
Multiple cohort studies have reported the operating characteristics of GM assay testing in pediatric patients undergoing therapy for acute leukemias or bone marrow transplantation (see Table 1). A number of these studies documented a sensitivity of the GM assay including the study with the largest pediatric patient population. One study with fewer total patients did not reveal high sensitivity for GM assay testing but this study was limited as it only included one identified case of IA. None of these studies included patients on routine antifungal prophylaxis and thus the results cannot be extrapolated to our patient population.
Only one study evaluating BG levels in children has been performed. This study was limited to healthy children and revealed elevated baseline levels of BG in a subset of the patients. To date, the Fungitell Assay testing has never been performed in immunocompromised pediatric patients.
Table 1. Operating characteristics of Galactomannan testing for diagnosis of proven or probable aspergillosis in pediatric patients
Author, Year
Total # patients in study
Proven or probable aspergillosis
Sensitivity
Specificity
TP
FP
TN
FN
Steinbach, 2007
64
1
0%
87%
0
8
55
1
Hovi, 2007
89
1
100%
93%
1
6
82
0
Sulaihan, 2001
347
9
100%
89.9%
9
34
304
0
Rohrlich, 1996
37
10
100%
92.6%
10
2
25
0
13.2.4 Gaps in knowledge
The Platelia Aspergillus EIA and the Fungitell Assay have each shown reassuring operating characteristics in adults making these biomarkers an attractive option for screening for IFI in children. More importantly, the 2 diagnostic tests afford the possibility of identifying an IFI days to weeks before the clinical diagnosis is made. However, it is not reasonable to extrapolate results from these adult studies to children. There is an absence of data regarding the operating characteristics of either biomarker in large homogeneous cohorts of children with leukemia.
Additionally, no data exist on either biomarker in a cohort of pediatric patients receiving antifungal prophylaxis. The use of prophylactic anti-fungal therapy will likely reduce the incidence of IFI or suppress actual IFI and thus potentially alter the predictive values of these biomarkers. As noted above, the use of prophylactic therapy will likely become standard of care and therefore it is imperative to define the operating characteristics of these biomarkers in such a population.
Lastly, it may be optimal to consider the results of each biomarker in combination as opposed to evaluating the impact of each study independently. The simultaneous interpretation of both Platelia Aspergillus EIA and the Fungitell Assay for the identification of IFI in children has never been evaluated. It is plausible that interpreting the 2 biomarkers in combination would improve the sensitivity of detecting an IFI.
13.2.5 Summary
Currently, the decision to start empiric antifungal therapy in pediatric patients with neutropenia in the setting of AML is based on the persistence of fever despite a number of days of broad spectrum antibiotics. This approach is rudimentary and likely not particularly sensitive for the presence of an IFI. Maartens et al, identified afebrile and asymptomatic adults with IFI, emphasizing the need for better diagnostic studies and abandoning the use of persistent or new fever as the only trigger for antifungal modification. The availability of the Platelia Aspergillus EIA and the Fungitell Assay offer an opportunity to more accurately stratify pediatric patients for their risk for breakthrough IFI while on antifungal prophylaxis. Adult trial data for both of these assays are encouraging as they are almost always correct when the results are negative (i.e., high NPV) and maintain a reasonable sensitivity for presence of IFI (i.e., high sensitivity). Certainly, they may be at risk for false positive results (i.e., low PPV) which could result in unnecessarily treating patients without an IFI. Despite this potential for overtreatment it is still likely more desirable to have such results guide empiric antifungal decisions as opposed to the limited current practice of persistent fever and neutropenia.
However, before we can employ these biomarker assays as guides for initiating or escalating to empiric antifungal therapy in children we must better define their operating characteristics in the same population. The parent study cohort provides a one time opportunity to evaluate the operating characteristics of both of these tests in the setting of 2 different antifungal prophylaxis agents in a homogeneous cohort of pediatric AML patients. The choice of which antifungal agent to use for future trials will likely be
determined by the results of this study. Knowledge of the operating characteristics of each biomarker interpreted separately and in combination under these study conditions is necessary to inform their potential utility as integral markers to guide empiric antifungal choices for future AML patients.
13.3 Specific Aims
Primary Aim:
i) To define the operating characteristics of 2 fungal antigen assays, Platelia Aspergillus EIA and Fungitell Assay for the identification of IA only and all IFI among pediatric AML patients receiving antifungal prophylaxis. This primary aim will have 3 sub-aims:
a) Define the test characteristics using a combination of the results from the Platelia Aspergillus EIA and Fungitell Assay for identifying IA only and all IFI.
Hypothesis: A positive Platelia Aspergillus EIA or positive Fungitell Assay will be more sensitive at identifying patients with IA only or with IFI while on antifungal prophylaxis as compared to either test alone.
b) Define the test characteristics of the Fungitell Assay for identifying all IFI.
Hypothesis: A single positive Fungitell Assay will have sensitivity in identifying all IFI in pediatric AML patients on antifungal prophylaxis.
c) Define the test characteristics of Platelia Aspergillus EIA for identifying IA only.
Hypothesis: A single positive Platelia Aspergillus EIA will have sensitivity in identifying IA only in pediatric AML patients on antifungal prophylaxis.
13.4 Patient Accrual
All patients enrolled on ACCL0933 will be offered the chance to participate in the anti-fungal screening study. We anticipate that at least of the patients in the parent trial will enroll in this ancillary study resulting in an estimated 440 patients at baseline. Those who consent will undergo Platelia Aspergillus EIA and Fungitell Assay testing. Blood sampling will be conducted twice weekly during anti-fungal prophylaxis treatment after each course of chemotherapy.
Each patient will have the potential for multiple courses of chemotherapy with each course having variable durations of neutropenia. Based on data from the AAML0531 trial, we have estimated the number of patients progressing from the first course of chemotherapy through the fourth course of therapy as well as duration of neutropenia for each course (see Table 2). Given a planned frequency of biomarker testing of twice per week, estimates of the number of Platelia Aspergillus EIA and Fungitell Assays performed during each chemotherapy course are provided (see Table 2).
Table 2. Estimated number of Platelia Aspergillus EIA and Fungitell Assay performed per course.
Chemotherapy course
Estimated Duration of neutropenia* (days)
# of testing time points for 1 patient during neutropenia!
Platelia EIA
Fungitell Assay
I ( )
20
6
2640
2640
II ( )
18
5
1900
1900
III ( )
17
5
1685
1685
IV ( )
28
8
1728
1728
Total
-
-
7953
7953
13.5 Gold Standards for IFI and IA Infections
The criteria established by the EORTC/MSG for proven or probable IFI and proven or probable IA will be used as the gold standard. These definitions have been used as the primary endpoints for prior studies validating Platelia Aspergillus EIA and the Fungitell Assay.
13.6 Methodology to Identify IFI and IA
The EORTC/MSG guidelines incorporate clinical, microbiologic, histopathologic, and radiographic data for classification of proven or probable IFI or IA. Therefore, in order to establish these diagnoses, the following data will be obtained (according to the IFI checklist (Section 10.2): pathology reports (including autopsy reports), CT scan and MRI reports, fungal gram stain and microbiology culture results, non-culture mycology testing results (i.e. histoplasma urine antigens, cryptococcal CSF and serum antigens), ophthalmology exams, and bronchoscopy reports. An independent data review committee including infectious disease and oncology experts who are unaware of treatment assignments will review and classify all cases of fungal infection according to the consensus criteria of the EORTC/MSG.
13.6.1 Justification of Methodologic Choices
13.6.1.1 Justification for Chosen Thresholds for Platelia Aspergillus EIA and Fungitell Assay
IFI outcomes are often devastating, thus it would be desirable to optimize sensitivity at the potential expense of specificity. Furthermore, a highly sensitive test will likely result in a high negative predictive value. Clinicians caring for patients with positive tests would then have a heightened concern for IFI while a negative test result would reassure them that no further modifications to antifungal therapy are necessary at that time. It was with these intentions that the following threshold values were chosen to conclude negative and positive results for each biomarker.
The level of GM index for Platelia Aspergillus EIA will be the established threshold to determine a positive result. This is the level that was established for FDA approval during testing in adults. The operating characteristics of this test have been evaluated in pediatric and adult patients using various cutoffs ranging from 0.5 to 1.5 as well as using single and consecutive positive results. Increasing the threshold level and requiring multiple consecutive positive results often reduced the sensitivity while optimizing specificity. As noted above, our goal is to optimize sensitivity and negative predictive value, at the risk of lower specificity and positive predictive value. Therefore, the lower threshold of on a single test was chosen.
The Fungitell Assay threshold result of was chosen based on manufacturer recommendations and available data. For two adult studies that evaluated this test, the cut-off for a positive test was lowered to Lowering of the manufacturer threshold in these two studies resulted in high sensitivity which would be consistent with the goals of our study. However, analysis of BG levels in 120 healthy children revealed that of them had BG levels greater than Although this level would optimize sensitivity, the likelihood for false positivity is too high. There were still of healthy children in this study that had a level of . This suggests that even at a level of , sensitivity of this assay in children would be preserved. Therefore, the manufacturer threshold of was chosen. For both biomarker assays, a post hoc analysis of various cutoffs as well as assessment of sequential positive testing will be performed in an attempt to identify the most ideal cut-off for future use of this assay as an integral biomarker (please see statistical analysis below).
13.6.1.2 Justification for IFI Gold Standard
We have chosen to use EORTC/MSG defined proven or probable IA or IFI (Appendix II) as the gold standard. The ideal gold standard to compare to each biomarker would be a positive culture of a fungal organism from blood or infected tissue. However, there are significant challenges to establish the presence of fungal infection with isolation of the etiologic organism. Certain molds such as Aspergillus
do not grow routinely in blood cultures, the ability to obtain tissue for culture can be impacted by the size and location of a visceral lesion, and the clinical status of a patient may preclude invasive procedures to obtain cultures. Therefore, an alternate endpoint to identify all patients who truly have IFI is necessary. This issue has been addressed by the EORTC/MSG. This group of experts initially created criteria based on clinical, radiographic and culture data to define possible, probable and proven IFI in 2002 and revised these criteria in 2009. These criteria have served as the primary endpoint for major trials of antifungal drug efficacy, in strategy trials, for formulating clinical practice guidelines, as well as for undertaking epidemiologic studies. Consistent use of these criteria as the primary endpoint will allow for comparison of the resultant data to prior and future studies.
13.7 Factors resulting in False Positive Results
A number of medications, medical interventions, and infections have been suggested as possible causes of false positive results for BG and GM testing. Table 3 lists the potential causes of false positive results reported in the literature. It is anticipated that patients being treated for AML will have reason to be exposed to a number of these medications, infusions and/or medical interventions. Additionally, Pneumocystis jiroveci infection is also considered a cause of a "false positive" BG test. Technically this is not a true false positive as the Fungitell Assay is detecting BG from the cell wall of Pneumocystis jiroveci as it would for other fungal infections. However, in this instance it is considered a false positive as the treatment of choice for this infection is trimethoprim-sulfamethoxazole as opposed to a typical anti-fungal agent. A sensitivity analysis (as described in Section 13.8.4 below) will be performed to investigate the impact of these false positive rates on the operating characteristics of the 2 biomarkers.
Table 3. Potential factors resulting in false positive testing for ( ) beta-D glucan and GM assays
Factor
( ) Beta-D Glucan Assay
Galactomannan EIA Assays
Medications
Amoxicillin-clavulanate
*Piperacillin-Tazobactam
*Amoxicillin-clavulanate
Infusions
*Intravenous immune globulin
*Cellulose filters for IV infusion
*Albumin
*Plasmalyte (electrolyte infusion)
*Intravenous solution with sodium gluconate
Medical interventions
*Hemodialysis with cellulose filter
*Gauze packing on serosal surfaces
*Enteral feeding with soybean proteins
Other infections
*Pneumocystis jiroveci
*Penicillium spp.
*Histoplasma capsulatum
*Geotrichum
*Neosartoria
13.8 Statistical Design
13.8.1 Sample Size and Estimated Event Rates
The parent trial comparing prophylaxis with caspofungin to fluconazole in newly diagnosed AML patients anticipates enrollment of at least 275 patients for each arm with a total cohort of approximately 550 patients. As noted above we anticipate that at least of the patients enrolled in the parent trial will also be enrolled in this ancillary study. This will result in 220 patients from each study arm. Consent for testing will be included as a part of the parent trial enrollment, thus significantly limiting the need for additional resources to complete this biomarker study.
The estimated number of probable or proven IFI events for final analyses will be different for both proposed biomarkers as they account for different types of fungal infections and the incidence for each will vary by study arm. The Fungitell Assay has the potential to identify most pathogenic fungi and thus a majority of the probable or proven IFIs will be considered as true events (excluding IFIs form Zygomycetes and Cryptococci). The Platelia Aspergillus EIA is specific for Aspergillus and thus only probable or proven IA will be considered as true events for that analysis.
Based on Section 9.3.3 of the parent trial the estimated incidence of IFI for patients in the fluconazole group is and in the caspofungin arm. Assuming the enrollment of 220 patients in each study arm, there would 18 IFI events in the fluconazole group and 4 IFI events in the caspofungin group. Based on data from the CCG 2961 AML trial, one-third of microbiologically proven fungal infection were the result of Aspergillus. Therefore, it is estimated that 6 of the 18 IFI events in the fluconazole group will be IA and between 1 and 2 of the IFI events in the caspofungin group will be IA.
13.8.2 Sensitivity, Specificity, PPV, and NPV
The validity of a biomarker is based on whether the study appropriately categorizes patients with and without the illness in question (sensitivity and specificity). Alternatively the validity of a test can be measured by how well the test results predict the presence or absence of the disease (PPV and NPV). Collectively, sensitivity, specificity, PPV, and NPV are often referred to as the test's operating characteristics with the sensitivity and NPV being the most clinically relevant parameters for this study. Each component of the operating characteristics will be calculated based first on the entire cohort. As indicated in the sample size estimates above the incidence of IFI will vary between the two study arms. It is well documented that variations in the incidence/prevalence of a disease will impact the operating characteristics of a diagnostic test specifically for the PPV and NPV. Therefore, each assay's sensitivity, specificity, PPV and NPV will also be calculated separately for each study arm.
The operating characteristics for both the Platelia Aspergillus EIA and the Fungitell Assay will be computed at the patient level for each of the sub-aims as follows:
a) Outcome of IA only or all IFI defined as a single positive test for either the Platelia Aspergillus EIA or the Fungitell Assay as compared to the EORTC/MSG criteria for proven or probable IA only or all IFI.
b) Outcome of IA only defined as a single positive test for Platelia Aspergillus EIA only as compared to the EORTC/MSG criteria for proven or probable IA only.
c) Outcome of all IFI defined as a single positive test for the Fungitell Assay as compared to the EORTC/MSG criteria for all proven or probable IFI.
Sensitivity, specificity, PPV and NPV and their accompanying confidence intervals will be calculated using STATA statistical software version 11.0 (College Station, TX). As noted above, these parameters will first be calculated for the entire cohort and then for each study arm separately. The latter analyses are important as the incidence of IFI may vary by study arm thus impacting the interpretation of the assay results. A patient with multiple episodes of IFI will only be included in the analyses as a single IFI.
13.8.3 Receiver Operator Characteristics Curve
In addition to understanding the operating characteristics of a diagnostic test at a single defined threshold, it is also important to understand how variations in the test's threshold can alter the test's operating characteristics. The receiver operating characteristics (ROC) curve is a useful approach to illustrate how these operating characteristics will change as the threshold changes. Therefore, a receiver-operating-
characteristics (ROC) curve will be generated with a series of sensitivities and specificities derived from various cutoff values. For the Platelia Aspergillus EIA cutoffs of and 2.0 will be used. For the Fungitell Assay cutoffs of , and will be used to create the ROC. The ROC curve will be displayed graphically (sensitivity vs. 1-specificity) and evaluated numerically (c-statistic). The c-statistic (also referred to as the area under the curve (AUC)) varies from 0.5 to 1.0 and is a measure of the test's ability to discriminate between patients with and without the gold standard diagnosis. A c-statistic of 0.5 is possible by chance alone while a perfectly discriminating test will result in a c-statistic of 1.0.
Additionally, the ROC curves will be used in an exploratory analysis to identify the threshold for each biomarker assay that optimizes the diagnostic test's sensitivity while maintaining a reasonable specificity. The identified thresholds will be used to categorize each patient as "likely to have IFI or IA" and "not likely to have IFI or IA". Once these 2 sub-groups are defined we will calculate the incidence rates of IFI or IA for each sub-group and compare them. Because the anticipated incidence for IFI and IA may be variable between the two study arms (those receiving fluconazole and those receiving caspofungin) this approach will have to be done at the level of each study arm. The incidence rates will be compared statistically using Pearson's Chi-square analysis.
Finally, to further explore the ideal utility and interpretation of each biomarker, serial testing results will be explored. For this analysis the Platelia Aspergillus EIA will be considered positive when a patient has 2 consecutive tests GM index and the Fungitell Assay will be considered positive when a patient has 2 consecutive test results . Operating characteristics and ROC curves will be constructed in a similar manner as discussed above.
13.8.4 Sensitivity Analysis
Sensitivity analyses will be explored for reasoning expressed in both Sections 13.1 and 13.7 above. The first sensitivity analysis will attempt to identify the direction and magnitude of the bias resulting from the availability of clinical BG and GM testing outside of the ancillary study. Such testing has the potential to change the treating clinician's approach for diagnosing an IFI. It is possible that these test results could result in more or less investigation (i.e., radiologic imaging) to identify an IFI which could ultimately impact on the incidence of identified IFI. Therefore, in addition to calculating the operating characteristics for all patients enrolled as described in Section 13.8.2 above, the same operating characteristics will be calculated after excluding all patients that had at least 1 biomarker test result available to the treating clinician.
The second sensitivity analysis will be performed to explore the impact of the various factors described in Section 13.7 that may contribute to a positive result for either biomarker. False positive results would impact the final interpretation of sensitivity and PPV for each of the assays. However, it is also possible that one of the factors listed in Table 3 is present in a patient that truly has an IFI. Therefore, we plan to still include all patients in the primary analysis for calculation of each assays' operating characteristics. In this sensitivity analysis, we will eliminate all patients with a positive test that correlates in time with at least 1 of the factors listed in Table 3.
13.9 Significance
Fungal infections continue to be major contributors to morbidity and mortality in children receiving chemotherapy for AML. Although antifungal prophylaxis in these patients will reduce the frequency of IFI, it will not eliminate the risk of these devastating infections. Early diagnosis and therapeutic modifications are paramount to improving patient outcomes. The Platelia Aspergillus EIA and the Fungitell Assay are potential diagnostic tools that could improve the time to diagnosis of IFIs. More definitive data regarding the operating characteristics of these 2 biomarkers interpreted simultaneously and separately in the setting of a large pediatric cohort receiving fungal prophylaxis are necessary.
Evaluating the biomarkers first as integrated tests will provide valuable information regarding the utility of each test so that they can be utilized as integral markers in future pediatric cancer trials. Finally, specimens from this study will be stored for potential future investigation. This will allow for the possibility of evaluating future versions of these or other biomarker assays for the identification of IFI in this cohort.
14.0 SPECIAL STUDIES SPECIMEN REQUIREMENTS
14.1 Single Nucleotide Polymorphisms (This study is optional)
Genotypes of interest in genes mediating immune function will be determined by review of experimental data from AAML0531 and review of the literature. Genotyping will be conducted as part of 1 R01 CA133881 and analysis will be performed on the Taqman Open Array Platform according to the manufacturer's instructions.
14.1.1 Sample Collection
Patients Enrolled on AAML1031:
All samples for ACCL0933 will be obtained from the AML Reference Laboratory from samples submitted on patients enrolled on AAML1031. Thus, no additional sample collection beyond AAML1031 sample collection will occur for patients enrolled on the AAML1031 trial.
All Other Patients:
For patients not enrolled on AAML1031, 5 mL of peripheral blood should be collected in a purple top tube at the end of Course I, when the patient has an ANC (and with no circulating blasts).
14.1.2 Labeling:
Label the tubes with the patient's COG ID number, protocol ID number, BPC #, date and time of collection.
14.1.3 Shipping:
Ship sample at room temperature, 2nd day delivery, using the COG courier account (https://members.childrensoncologygroup.org/_files/reference/FEDEXmemo.pdf). The laboratory is unable to accept Saturday deliveries. Include a COG Specimen Transmittal Form with shipment.
The SNP sample (for patients not enrolled on AAML1031) should be shipped to the address below.
Please contact Dr. Richard Aplenc for any questions regarding sample acquisition.
15.0 BANKING SPECIMENS
If the patient consents, leftover blood samples (from the studies described in Section 13 and 14) will be banked for future research studies.
APPENDIX I: YOUTH INFORMATION SHEETS
INFORMATION SHEET REGARDING RESEARCH STUDY ACCL0933
(for children from 7 through 12 years of age)
A Research Study Comparing 2 Drugs Used To Prevent Serious Fungal Infections In Children With Acute Myeloid Leukemia.
We have been talking with you about your likelihood of getting Invasive Fungal Infections. Invasive Fungal Infections are infections which occur in people whose natural infection-fighting ability (also called immunity) have been reduced. The strong cancer fighting drugs (called chemotherapy) used to treat your acute myeloid leukemia (AML) reduce your immunity and make you likely to get invasive fungal infections.
We are asking you to take part in a research study because you are at risk of invasive fungal infections. A research study is when doctors work together to try out new ways to help people who are sick. In this study, we are trying to find better ways to prevent invasive fungal infections in children on treatment for AML.
Children who are part of this study will be given medicines that help prevent invasive fungal infections. These drugs are called antifungal agents. In this study, one group of children will get the usual antifungal drug called fluconazole. The other group will get a newer antifungal agent called caspofungin. Your doctor will tell you which group you are in. We do not know if the newer antifungal agent will be better than the usual treatment. That is why we are doing this study.
Sometimes good things can happen to people when they are in a research study. These good things are called "benefits." We hope that a benefit to you of being part of this study is a better chance of avoiding invasive fungal infections during your treatment for AML, but we don't know for sure if there is any benefit of being part of this study.
Sometimes bad things can happen to people when they are in a research study. These bad things are called "risks." There is a risk that you will have bad effects from the newer antifungal agent or that it will not be better at preventing you from getting invasive fungal infections during your treatment for AML. Other things may happen to you that we don't yet know about.
Your family can choose to be part of this study or not. Your family can also decide to stop being in this study at any time once you start. There may be other treatments for your illness that your doctor can tell you about. Make sure to ask your doctors any questions that you have.
We are asking your permission to collect additional blood for some special tests. We want to see if 2 new blood tests can help doctors detect fungal infections as early as possible, and better than the usual tests used. We also want extra blood samples for another special blood test that looks at your genes for an abnormality that may make an individual more likely to get invasive fungal infections. Samples for these tests would be taken when other standard blood tests are being performed, so there would be no extra procedures. You can still take part in this study even if you don't allow us to collect the extra blood samples for research.
INFORMATION SHEET REGARDING RESEARCH STUDY ACCL0933 (for teens from 13 through 17 years of age)
A Research Study Comparing 2 Drugs Used To Prevent Serious Fungal Infections In Children and Adolescents With Acute Myeloid Leukemia.
We have been talking with you about your likelihood of getting Invasive Fungal Infections. Invasive Fungal Infections are infections which occur in people whose natural infection-fighting ability (also called immunity) have been reduced. The strong cancer fighting drugs (called chemotherapy) used to treat your acute myeloid leukemia (AML) reduce your immunity and make you likely to get invasive fungal infections.
We are asking you to take part in a research study because you are at risk of invasive fungal infections. A research study is when doctors work together to try out new ways to help people who are sick. In this study, we are trying to find better ways to prevent invasive fungal infections in children on treatment for AML.
Children who are part of this study will be given medicines that help prevent invasive fungal infections. These drugs are called antifungal agents. Children and adolescents that are part of this study will be placed into 1 of 2 treatment groups by a process called randomization. Randomization means that the study treatment groups are assigned by chance, and is like flipping a coin, only it is done by a computer. In this study, one group of children will get the usual antifungal drug called fluconazole. The other group will get a newer antifungal agent called caspofungin. Your doctor will tell you which group you are in. We do not know if the newer antifungal agent will be better than the usual treatment at preventing invasive fungal infections. That is why we are doing this study.
Sometimes good things can happen to people when they are in a research study. These good things are called "benefits." We hope that a benefit to you of being part of this study is a better chance of avoiding invasive fungal infections during your treatment for AML, but we don't know for sure if there is any benefit of being part of this study.
Sometimes bad things can happen to people when they are in a research study. These bad things are called "risks." There is a risk that you will have bad effects from the newer antifungal agent or that it will not be better at preventing you from getting invasive fungal infections during your treatment for AML. Other things may happen to you that we don't yet know about.
Your family can choose to be part of this study or not. Your family can also decide to stop being in this study at any time once you start. There may be other treatments for your illness that your doctor can tell you about. Make sure to ask your doctors any questions that you have.
We are asking your permission to collect additional blood for some special tests. We want to see if 2 new blood tests can help doctors detect fungal infections as early as possible, and better than the usual tests used. These new tests are called beta-D glucan and galactomannan assays. We also want extra blood samples for another special blood test that looks at your genes for an abnormality that may make an individual more likely to get invasive fungal infections. This is called single nucleotide polymorphism (SNP) analysis. Samples for these tests would be taken when other standard blood tests are being performed, so there would be no extra procedures. You can still take part in this study even if you don't allow us to collect the extra blood samples for research.
APPENDIX II: EORTC/MSG CRITERIA
Criteria for proven invasive fungal disease except for endemic mycoses
Analysis and specimen
Molds
Yeasts
Microscopic analysis: sterile material
Histopathologic, cytopathologic, or direct microscopic examination of a specimen obtained by needle aspiration or biopsy in which hyphae or melanized yeast-like forms are seen accompanied by evidence of associated tissue damage
Histopathologic, cytopathologic, or direct microscopic examination of a specimen obtained by needle aspiration or biopsy from a normally sterile site (other than mucous membranes) showing yeast cells-for example, Cryptococcus species indicated by encapsulated budding yeasts or Candida species showing pseudohyphae or true hyphae
Culture
Sterile material
Recovery of a mold or "black yeast" by culture of a specimen obtained by a sterile procedure from a normally sterile and clinically or radiologically abnormal site consistent with an infectious disease process, excluding bronchoalveolar lavage fluid, a cranial sinus cavity specimen, and urine
Recovery of a yeast by culture of a sample obtained by a sterile procedure (including a freshly placed [!24 h ago] drain) from a normally sterile site showing a clinical or radiological abnormality consistent with an infectious disease process
Blood
Blood culture that yields a mold (e.g., Fusarium species) in the context of a compatible infectious disease process
Blood culture that yields yeast (e.g., Cryptococcus or Candida species) or yeast-like fungi (e.g., Trichosporon species)
Serological analysis: CSF
Not applicable
Cryptococcal antigen in CSF indicates disseminated cryptococcosis
Criteria for probable invasive fungal disease except for endemic mycoses
Host factors \({ }^{\text {a }}\)
Recent history of neutropenia ( \(<0.5 \times 10^{9}\) neutrophils/ \(L \left[<500\right.\) neutrophils/ \(\left.mm ^{3}\right]\) for \(>10\) days) temporally related to the onset
of fungal disease
Receipt of an allogeneic stem cell transplant
Prolonged use of corticosteroids (excluding among patients with allergic bronchopulmonary aspergillosis) at a mean minimum
dose of \(0.3 mg / kg /\) day of prednisone equivalent for \(>3\) weeks
Treatment with other recognized T cell immunosuppressants, such as cyclosporine, TNF- \(\alpha\) blockers, specific monoclonal
antibodies (such as alemtuzumab), or nucleoside analogues during the past 90 days
Inherited severe immunodeficiency (such as chronic granulomatous disease or severe combined immunodeficiency)
Clinical criteria \({ }^{\text {b }}\)
Lower respiratory tract fungal disease \({ }^{\text {c }}\)
The presence of 1 of the following 3 signs on CT:
Dense, well-circumscribed lesions(s) with or without a halo sign
Air-crescent sign
Cavity
Tracheobronchitis
Tracheobronchial ulceration, nodule, pseudomembrane, plaque, or eschar seen on bronchoscopic analysis
Sinonasal infection
Imaging showing sinusitis plus at least 1 of the following 3 signs:
Acute localized pain (including pain radiating to the eye)
Nasal ulcer with black eschar
Extension from the paranasal sinus across bony barriers, including into the orbit
CNS infection
1 of the following 2 signs:
Focal lesions on imaging
Meningeal enhancement on MRI or CT
Disseminated candidiasis \({ }^{ d }\)
At least 1 of the following 2 entities after an episode of candidemia within the previous 2 weeks:
Small, target-like abscesses (bull's-eye lesions) in liver or spleen
Progressive retinal exudates on ophthalmologic examination
Mycological criteria
Direct test (cytology, direct microscopy, or culture)
Mold in sputum, bronchoalveolar lavage fluid, bronchial brush, or sinus aspirate samples, indicated by 1 of the following:
Presence of fungal elements indicating a mold
Recovery by culture of a mold (e.g., Aspergillus, Fusarium, Zygomycetes, or Scedosporium species)
Indirect tests (detection of antigen or cell-wall constituents) \({ }^{\text {e }}\)
Aspergillosis
Galactomannan antigen detected in plasma, serum, bronchoalveolar lavage fluid, or CSF
Invasive fungal disease other than cryptococcosis and zygomycoses
\(\beta\)-D-glucan detected in serum
REFERENCES
Groll AH, Kurz M, Schneider W, et al: Five-year-survey of invasive aspergillosis in a paediatric cancer centre. Epidemiology, management and long-term survival. Mycoses 42:431-42, 1999
McNeil MM, Nash SL, Hajjeh RA, et al: Trends in mortality due to invasive mycotic diseases in the United States, 1980-1997. Clin Infect Dis 33:641-7, 2001
Edmond MB, Wallace SE, McClish DK, et al: Nosocomial bloodstream infections in United States hospitals: a three-year analysis. Clin Infect Dis 29:239-44, 1999
Martin GS, Mannino DM, Eaton S, et al: The epidemiology of sepsis in the United States from 1979 through 2000. N Engl J Med 348:1546-54, 2003
Watson RS, Carcillo JA, Linde-Zwirble WT, et al: The epidemiology of severe sepsis in children in the United States. Am J Respir Crit Care Med 167:695-701, 2003
Zaoutis TE, Argon J, Chu J, et al: The epidemiology and attributable outcomes of candidemia in adults and children hospitalized in the United States: a propensity analysis. Clin Infect Dis 41:1232-9, 2005
Lin S-J, Schranz J, Teutsch. SM: Aspergillosis case-fatality rate: systemic review of the literature. Clinical Infectious Diseases 32:358-66, 2000
Walmsley S, Devi S, King S, et al: Invasive Aspergillus infections in a pediatric hospital: a tenyear review. Pediatr Infect Dis J 12:673-82, 1993
Abbasi S, Shenep JL, Hughes WT, et al: Aspergillosis in children with cancer: A 34-year experience. Clin Infect Dis 29:1210-9, 1999
Hovi L, Saarinen-Pihkala UM, Vettenranta K, et al: Invasive fungal infections in pediatric bone marrow transplant recipients: single center experience of 10 years. Bone Marrow Transplant 26:999-1004, 2000
Burgos A, Zaoutis TE, Dvorak CC, et al: Pediatric invasive aspergillosis: a multicenter retrospective analysis of 139 contemporary cases. Pediatrics 121:e1286-94, 2008
Sung L, Lange BJ, Gerbing RB, et al: Microbiologically documented infections and infectionrelated mortality in children with acute myeloid leukemia. Blood 110:3532-9, 2007
Robenshtok E, Gafter-Gvili A, Goldberg E, et al: Antifungal prophylaxis in cancer patients after chemotherapy or hematopoietic stem-cell transplantation: systematic review and meta-analysis. J Clin Oncol 25(34):5471-5489, 2007
Guidelines for preventing opportunistic infections among hematopoietic stem cell transplant recipients. Recommendations of CDC, the Infectious Disease Society of America, and the American Society of Blood and Marrow Transplantation. Cytotherapy 3(1):41-54, 2001
Maertens J: Evaluating prophylaxis of invasive fungal infections in patients with haematologic malignancies. Eur J Haematol 78(4):275-282, 2007
Goodman JL, Winston DJ, Greenfield RA, et al: A controlled trial of fluconazole to prevent fungal infections in patients undergoing bone marrow transplantation. N Engl J Med 326:845-51, 1992
Kanda Y, Yamamoto R, Chizuka A, et al: Prophylactic action of oral fluconazole against fungal infection in neutropenic patients. A meta-analysis of 16 randomized, controlled trials. Cancer 89:1611-25, 2000
Wingard JR: Design issues in a prospective randomized double-blinded trial of prophylaxis with fluconazole versus voriconazole after allogeneic hematopoietic cell transplantation. Clin Infect Dis 39 Suppl 4:S176-180, 2004
Lehrnbecher T, Ethier MC, Zaoutis T, et al: International variations in infection supportive care practices for paediatric patients with acute myeloid leukaemia. Br J Haematol 147:125-8, 2009
Wingard J: Results of a randomized, double-blind trial of fluconazole (FLU) vs. voriconazole (VORI) for the prevention of invasive fungal infections (IFI) in 600 allogeneic blood and marrow transplant (BMT) patients. Blood 110(Abstract 163):55a-56a, 2007
Mattiuzzi G: Intravenous voriconazole (IV-VORI) prevents invasive fungal infections (IF) in patients with acute myelogenous leukemia (AML) and high-risk myelodysplastic syndrome. Paper presented at: 46th American Society of Hematology Annual Meeting; San Diego, CA., 2004
Walsh TJ, Pappas P, Winston DJ, et al: Voriconazole compared with liposomal amphotericin B for empirical antifungal therapy in patients with neutropenia and persistent fever. N Engl J Med 346(4):225-234, 2002
Walsh TJ, Lutsar I, Driscoll T, et al: Voriconazole in the treatment of aspergillosis, scedosporiosis and other invasive fungal infections in children. Pediatr Infect Dis J 21:240-8, 2002
Johnson LB, Kauffman CA: Voriconazole: a new triazole antifungal agent. Clin Infect Dis 36:630-7, 2003
Cornely OA, Maertens J, Winston DJ, et al: Posaconazole vs. fluconazole or itraconazole prophylaxis in patients with neutropenia. N Engl J Med 356:348-59, 2007
van Burik JA, Ratanatharathorn V, Stepan DE, et al: Micafungin versus fluconazole for prophylaxis against invasive fungal infections during neutropenia in patients undergoing hematopoietic stem cell transplantation. Clin Infect Dis 39:1407-16, 2004
Seibel NL, Schwartz C, Arrieta A, et al: Safety, tolerability, and pharmacokinetics of Micafungin (FK463) in febrile neutropenic pediatric patients. Antimicrob Agents Chemother 49:3317-24, 2005
Denning DW, Marr KA, Lau WM, et al: Micafungin (FK463), alone or in combination with other systemic antifungal agents, for the treatment of acute invasive aspergillosis. J Infect 53:337-49, 2006
Stingl H, Chandramouli V, Schumann WC, et al: Changes in hepatic glycogen cycling during a glucose load in healthy humans. Diabetologia 49:360-8, 2006
Zaoutis TJH, Huang L, et al: Prospective Mulitcenter Study of Caspofungin for the treatment of documented fungal infections in pediatric patients. Infectious Diseases Society of America 45th Annual Meeting; San Diego, CA., 2008
Walsh TJ, Teppler H, Donowitz GR, et al: Caspofungin versus liposomal amphotericin B for empirical antifungal therapy in patients with persistent fever and neutropenia. N Engl J Med 351:1391-402, 2004
Zaoutis TLT, Groll A, et al e: Safety Experience with Caspofungin in Pediatric Patients. Pediatric Academic Societies Annual Meeting; Honolulu, HI. 2008
Assessment Report for Mycamine. European Medicines Agency EMEA/CHMP/121708/2008, 2008
Pfeiffer CD, Fine JP, Safdar N: Diagnosis of invasive aspergillosis using a galactomannan assay: a meta-analysis. Clin Infect Dis 42:1417-27, 2006
Ostrosky-Zeichner L, Alexander BD, Kett DH, et al: Multicenter clinical evaluation of the (1->3) beta-D-glucan assay as an aid to diagnosis of fungal infections in humans. Clin Infect Dis 41:654-9, 2005
Rex JH: Galactomannan and the diagnosis of invasive aspergillosis. Clin Infect Dis 42:1428-30, 2006
Kwiatkowski D: Science, medicine, and the future: susceptibility to infection. BMJ 321:1061-5, 2000
Haralambous E, Weiss HA, Radalowicz A, et al: Sibling familial risk ratio of meningococcal disease in UK Caucasians. Epidemiol Infect 130:413-8, 2003
Sorensen TI, Nielsen GG, Andersen PK, et al: Genetic and environmental influences on premature death in adult adoptees. N Engl J Med 318:727-32, 1988
Foster CB, Chanock SJ: Mining variations in genes of innate and phagocytic immunity: current status and future prospects. Curr Opin Hematol 7:9-15, 2000
Choi EH, Foster CB, Taylor JG, et al: Association between chronic disseminated candidiasis in adult acute leukemia and common IL4 promoter haplotypes. J Infect Dis 187:1153-6, 2003
van der Poll T: Immunotherapy of sepsis. Lancet Infect Dis 1:165-74, 2001
Jurevic RJ, Bai M, Chadwick RB, et al: Single-nucleotide polymorphisms (SNPs) in human betadefensin 1: high-throughput SNP assays and association with Candida carriage in type I diabetics and nondiabetic controls. J Clin Microbiol 41:90-6, 2003
Schwartz GJ, Gauthier B: A simple estimate of glomerular filtration rate in adolescent boys. J Pediatr 106:522-6, 1985
Child CG, Turcotte JG: Surgery and portal hypertension. In: The liver and portal hypertension. Edited by CG Child. Philadelphia: Saunders:50-64, 1964
Pugh RN, Murray-Lyon IM, Dawson JL, et al: Transection of the oesophagus for bleeding oesophageal varices. The British journal of surgery 60 (8):646-9, 1973
De Pauw B, Walsh TJ, Donnelly JP, et al: Revised definitions of invasive fungal disease from the European Organization for Research and Treatment of Cancer/Invasive Fungal Infections Cooperative Group and the National Institute of Allergy and Infectious Diseases Mycoses Study Group (EORTC/MSG) Consensus Group. Clin Infect Dis 46:1813-21, 2008
Schulgen G, Olschewski M, Krane V, et al: Sample sizes for clinical trials with time-to-event endpoints and competing risks. Contemp Clin Trials 26:386-96, 2005
Latouche A, Porcher R, Chevret S: Sample size formula for proportional hazards modelling of competing risks. Stat Med 23:3263-74, 2004
Gray RA: Class of K-sample tests for comparing the cumulative incidence of a competing risk. The annals of Stat 16:1141-54, 1988
Stephens M, Smith NJ, Donnelly P: A new statistical method for haplotype reconstruction from population data. Am J Hum Genet 68:978-89, 2001
Stephens M, Donnelly P: A comparison of bayesian methods for haplotype reconstruction from population genotype data. Am J Hum Genet 73:1162-9, 2003
Benjamini Y, Drai D, Elmer G, et al: Controlling the false discovery rate in behavior genetics research. Behav Brain Res 125:279-84, 2001
DeMets DL, Lan KK: Interim analysis: the alpha spending function approach. Stat Med 13:134152; discussion 1353-6, 1994
Segal BH, Almyroudis NG, Battiwalla M, et al: Prevention and early treatment of invasive fungal infection in patients with cancer and neutropenia and in stem cell transplant recipients in the era of newer broad-spectrum antifungal agents and diagnostic adjuncts. Clin Infect Dis 44:402-9, 2007
Kaya Z, Gursel T, Kocak U, et al: Invasive fungal infections in pediatric leukemia patients receiving fluconazole prophylaxis. Pediatr Blood Cancer 52:470-5, 2009
Kusuki S, Hashii Y, Yoshida H, et al: Antifungal prophylaxis with micafungin in patients treated for childhood cancer. Pediatr Blood Cancer 53:605-9, 2009
Marty FM, Koo S: Role of (1-->3)-beta-D-glucan in the diagnosis of invasive aspergillosis. Med Mycol 47 Suppl 1:S233-40, 2009
Wheat LJ, Walsh TJ: Diagnosis of invasive aspergillosis by galactomannan antigenemia detection using an enzyme immunoassay. Eur J Clin Microbiol Infect Dis 27:245-51, 2008
Maertens J, Verhaegen J, Lagrou K, et al: Screening for circulating galactomannan as a noninvasive diagnostic tool for invasive aspergillosis in prolonged neutropenic patients and stem cell transplantation recipients: a prospective validation. Blood 97:1604-10, 2001
Leeflang MM, Debets-Ossenkopp YJ, Visser CE, et al: Galactomannan detection for invasive aspergillosis in immunocompromized patients. Cochrane Database Syst Rev:CD007394, 2008
Odabasi Z, Mattiuzzi G, Estey E, et al: Beta-D-glucan as a diagnostic adjunct for invasive fungal infections: validation, cutoff development, and performance in patients with acute myelogenous leukemia and myelodysplastic syndrome. Clin Infect Dis 39:199-205, 2004
Ellis M, Al-Ramadi B, Finkelman M, et al: Assessment of the clinical utility of serial beta-Dglucan concentrations in patients with persistent neutropenic fever. J Med Microbiol 57:287-95, 2008
Hovi L, Saxen H, Saarinen-Pihkala UM, et al: Prevention and monitoring of invasive fungal infections in pediatric patients with cancer and hematologic disorders. Pediatr Blood Cancer 48:28-34, 2007
Sulahian A, Boutboul F, Ribaud P, et al: Value of antigen detection using an enzyme immunoassay in the diagnosis and prediction of invasive aspergillosis in two adult and pediatric hematology units during a 4-year prospective study. Cancer 91:311-8, 2001
Rohrlich P, Sarfati J, Mariani P, et al: Prospective sandwich enzyme-linked immunosorbent assay for serum galactomannan: early predictive value and clinical use in invasive aspergillosis. Pediatr Infect Dis J 15:232-7, 1996
Smith PB, Benjamin DK, Jr., Alexander BD, et al: Quantification of 1,3-beta-D-glucan levels in children: preliminary data for diagnostic use of the beta-glucan assay in a pediatric setting. Clin Vaccine Immunol 14:924-5, 2007
Maertens J, Theunissen K, Verhoef G, et al: Galactomannan and computed tomography-based preemptive antifungal therapy in neutropenic patients at high risk for invasive fungal infection: a prospective feasibility study. Clin Infect Dis 41(9):1242-50, 2005
Herbrecht R, Letscher-Bru V, Oprea C, et al: Aspergillus galactomannan detection in the diagnosis of invasive aspergillosis in cancer patients. J Clin Oncol 20:1898-906, 2002
Marty FM, Lowry CM, Lempitski SJ, et al: Reactivity of ( )-beta-d-glucan assay with commonly used intravenous antimicrobials. Antimicrob Agents Chemother 50:3450-3, 2006
Cook NR: Statistical evaluation of prognostic versus diagnostic models: beyond the ROC curve. Clin Chem 54:17-23, 2008
This model informed consent form has been reviewed by the DCT/NCI and is the official consent document for this study. Institutions should use the sections of this document which are in bold type in their entirety. Editorial changes to these sections may be made as long as they do not change information or intent. If the local IRB insists on making deletions or more substantive modifications to any of the sections in bold type, they must be justified in writing by the investigator at the time of the institutional audit.
SAMPLE RESEARCH INFORMED CONSENT/PARENTAL PERMISSION FORM
ACCL0933
A Randomized Open-Label Trial of Caspofungin versus Fluconazole to Prevent Invasive Fungal Infections in Children Undergoing Chemotherapy for Acute Myeloid Leukemia (AML)
If you are a parent or legal guardian of a child who may take part in this study, permission from you is required. The assent (agreement) of your child may also be required. When we say "you" in this consent form, we mean you or your child; "we" means the doctors and other staff.
Why am I being invited to take part in this study?
You are being asked to take part in this research study because you are getting treatment with strong cancer fighting drugs (called chemotherapy) for AML, and therefore at risk of getting an invasive fungal infection.
Invasive fungal infections are infections caused by organisms called fungi that enter the blood stream and spread to different organs in the body. Chemotherapy used to treat AML severely reduces the body's natural infection fighting ability. In patients who died from infections while receiving treatment for AML, an invasive fungal infection was the cause in more than half of the cases. Preventing invasive fungal infections due to chemotherapy is therefore very important for the treatment success of people with AML.
This study is called a clinical trial. A clinical trial is a research study involving treatment of a disease in human patients. This study is organized by Children's Oncology Group (COG). COG is an international research group that conducts clinical trials for children with cancer. More than 200 hospitals in North America, Australia, New Zealand, and Europe are members of COG.
It is common to enroll children and adolescents with cancer in a clinical trial that seeks to improve cancer treatment over time. Clinical trials include only people who choose to take part. You have a choice between a standard preventive treatment for invasive fungal infections and this clinical trial.
Please take your time to make your decision. You may want to discuss it with your friends and family. We encourage parents to include their child in the discussion and decision to the extent that the child is able to understand and take part.
What is the current standard of treatment for this disease?
The current standard preventive treatment for people who are at risk of invasive fungal infections due to chemotherapy treatment for cancers like AML is the use of fungi fighting drugs (called antifungal therapy). The current standard antifungal drug used is called fluconazole.
Why is this study being done?
Current standard antifungal therapy with fluconazole (also called Diflucan ) has been shown to be effective in preventing invasive fungal infections in people with AML; especially those caused by the fungi Candida. However, previous studies have shown that it does not fully prevent infections caused by some types of fungi called filamentous fungi. Aspergillus is a type of filamentous fungi.
In this study, researchers want to find out if using a newer antifungal drug called caspofungin (also called Cancidas ) will be better than the current standard antifungal drug fluconazole at preventing invasive fungal infections when given to people with AML after receiving chemotherapy treatment.
The drug caspofungin was chosen because this class of medication has been shown to be effective in the prevention of various fungal infections, including Candida and Aspergillus, in a study of both adults and children. Caspofungin is an antifungal drug that has been approved by the Food and Drug Administration (FDA) for use in children as well as adults.
The use of caspofungin to prevent invasive fungal infections is experimental.
The overall goal of this study is to:
Compare the effects, good and/or bad, of 2 antifungal drugs: caspofungin and fluconazole on people getting treatment for AML, who are at risk of getting invasive fungal infections, to find out which is better. In this study, you will get either caspofungin or fluconazole. You will not get both.
What will happen on this study that is research?
Before you take part in this study, you will first get cancer treatment for AML that includes the use of chemotherapy. Taking part in this study will not change the cancer treatment plan you get.
Treatment on this study involves antifungal drugs used to prevent invasive fungal infections. In this study you will get 1 of 2 treatment plans. The 2 treatment arms are called:
Fluconazole Arm - Current standard treatment; patients will get therapy with fluconazole.
Caspofungin Arm - Experimental treatment; patients will get therapy with caspofungin.
Random Assignment
You will receive 1 of 2 different treatment plans. The treatment plan that you receive is decided by a process called randomization. Randomization means that the treatment is assigned based on chance. It is a lot like flipping a coin, except that it is done by computer. You and your doctor will not pick which treatment you get. You will have an equal chance of being on either the caspofungin arm or the fluconazole arm. The randomization process is described in the COG Family Handbook for Children with Cancer.
Subjects (people who agree to be part of this study) will have started treatment for AML. At the end of the first course of chemotherapy, some subjects will be randomized to receive fluconazole while others will get caspofungin. For the remainder of your AML chemotherapy, you will continue to get either caspofungin or fluconazole at the end of each chemotherapy course to prevent you from developing an invasive fungal infection.
Diagram of Treatment
This chart shows the treatments on the study.
Treatment Plan Tables
Preventive treatment that is standard for invasive fungal infections as well as standard tests and procedures are described in Attachment #1. The following drug therapies relate to the experimental comparison of the treatment groups in this study.
Various methods are used to give drugs:
IV - Drug is given using a needle or tubing inserted into a vein. Drugs can be given rapidly over a few minutes ("push") or slowly over minutes or hours ("infusion").
PO- Drug is given by tablet or liquid swallowed through the mouth.
Treatment for participants who are on Fluconazole Arm - Standard Treatment
Drug
How the drug will be given
Days
Fluconazole
IV Infusion over 1-2 hours (or
longer) or PO
Start at the end of each chemotherapy
course & continue until blood cells recover
or the next chemotherapy course begins.
Treatment for participants who are on Caspofungin Arm - Experimental Treatment
Drug
How the drug will be given
Days
Caspofungin
IV Infusion over 1 hour
Start at the end of each chemotherapy
(Dose on first day is different from
course & continue until blood cells recover
dose given in the days that follow)
or the next chemotherapy course begins.
Research Study Procedures
If you have a fungal infection while you are on this study, copies of some of the scans or reports of the tests that identify the infection will be sent to a central review center as part of COG quality control.
Optional Research Study Tests
We would like to do the following tests because you are a part of this study. These tests are not part of standard care and you do not need to take part in these tests to be on this study. The results of these tests will not be returned to you and no treatment decisions will be based on the results. The results of these tests will not be a part of your medical record. If you provide specimens to the researchers, there are no plans for you to profit from any new products developed from research done on your specimens.
At the end of this consent, there are questions for you to indicate if you want to take part in these optional research tests.
Researchers would like to see if they can identify certain biomarkers in the blood. Biomarkers are substances in the blood produced from the fungal organisms that cause invasive fungal infections. The biomarkers that will be measured in your blood are called galactomannan and beta-D-glucan. Findings from this research will help researchers know more about fungal infections, as well how to diagnose and treat them better.
If you agree, about a teaspoon of blood will be taken from you twice a week while you are receiving antifungal treatment. This will be drawn from your central line when other standard lab tests are being collected.
Single Nucleotide Polymorphisms (SNP) Analysis - Genetic Study
Researchers would like to look for genetic changes that may put subjects at an increased risk of invasive fungal infections. This test is called single nucleotide polymorphism (SNP) analysis. Information learned from this study may be useful in the future for identifying patients that are more likely to have invasive fungal infections.
[For subjects not enrolled on AAML1031]:
If you agree, about a teaspoon of blood will be collected for SNP analysis. The sample will be collected after the first course of chemotherapy when other routine blood tests are performed.
[For subjects enrolled on AAML1031]:
Since you are being treated on the AML clinical trial AAML1031, a blood sample will be sent to a COG laboratory after the first course of chemotherapy. If you agree, this sample can also be used for the SNP analysis and no extra blood will be collected.
Future Studies:
If you agree, we would like to store (bank) any leftover blood for future studies. The research that may be done with the samples is not designed to help you during your present treatment. It might help people who have cancer and other diseases in the future.
Research on the banked specimens is very unlikely to discover results that are important to your current or future health. However, if it does, COG will try to contact your doctor about what the research tests might mean. Only the doctor will be notified and the information will not
become part of your medical record. Your doctor will decide whether to discuss the results with you. Your doctor may recommend repeat testing, meeting with a genetic counselor, or no further action.
What side effects or risks can I expect from being in the study?
Treatment Risks
You may have side effects while on this study. All people taking part in this study will be carefully monitored for side effects. Side effects may be mild or very serious; and you may be given care to lessen side effects. Many side effects go away soon after you stop taking the drug causing the side effects, but in some cases, may last longer or never go away.
The risks of the individual drug given as standard treatment are listed in Attachment #2.
Reproductive risks: Women should not become pregnant and men should not father a baby while on this study because the drug(s) in this study can be bad for an unborn baby. If you or your partner can get pregnant, it is important for you to use birth control or not have sex while on this study. Check with your study doctor about what kind of birth control methods to use and how long to use them. Some birth control methods might not be approved for use in this study. Women should not breastfeed a baby while on this study. Also check with your doctor about how long you should not breastfeed after you stop the study treatment(s).
Risks of Study
Several studies have shown that even though fluconazole is effective in preventing fungal infections caused by Candida, it is not quite as effective at preventing fungal infections caused by filamentous fungi like Aspergillus. Infections with Aspergillus are usually very severe, and have been shown to cause more infection-related deaths than infections with Candida.
The use of caspofungin may cause more complications than the use of fluconazole.
The caspofungin treatment that is being studied could be less effective than the current standard treatment with fluconazole.
In addition to the risks described above, there may be unknown risks, or risks that we did not anticipate, associated with being in this study.
Risks and side effects reported or expected with caspofungin include:
Likely
May happen in 21 to 100 subjects out of every 100.
Less Likely
May happen in 20 or less than 20 subjects out of every 100.
Rare but serious
- Fever (high temperature)
- Chills
- Rash
- Diarrhea
- Reaction that can occur during or following infusion of
- Fluid build-up in the tissues of the arms and legs
- Pain and inflammation in the vein through which the drug was given
- Nausea
- Vomiting
- Pain in the abdomen (belly)
- Allergic reaction which can be life-threatening and potentially fatal. This reaction requires immediate medical treatment. It may include fever, chills and skin rash. Less commonly wheezing, shortness of breath, swelling of the
the drug. The reaction may include fever, chills, reddening of the face with feelings of warmth, rash, low or high blood pressure, fast heartbeat, fast breathing, and difficulty breathing
- Low level of potassium in the blood which may cause weakness, tiredness, muscle cramps, constipation, and abnormal heart beat and may require that you take extra potassium by mouth or through the vein
- Cough
- Redness of the skin
- Headache
- Low blood pressure
- Increase in the blood of certain enzymes or bilirubin (a substance that comes from the liver breaking down waste products) which could indicate liver irritation or damage
- Infection in the lung (pneumonia)
- Pain, fluid build-up and itching at the injection site
- Itching
- Fast or slow heart beat
- High blood pressure
- Bloating of the abdomen (belly)
- Constipation
- Acid or upset stomach (heartburn)
- Loss of desire to eat or appetite
- A feeling of weakness and/or tiredness
- Sleepiness
- Dizziness
- Tremor (shakiness usually of the hands)
- Reddening of the face with feelings of warmth
- Fewer white blood cells, red blood cells and platelets in the blood
○ a low number of white blood cells can make it easier to get infections
○ a low number of red blood cells can make you feel tired and weak
- a low number of platelets causes you to bruise and bleed more easily
- Fever with a low white blood cell count which could indicate infection and may require hospitalization and treatment with antibiotics
- Abnormal clotting of the blood
- Inflammation of mucosal tissues like the lining of the
throat, drop in blood pressure, and rapid heart rate may occur.
- A life-threatening condition in which the level of oxygen in the blood becomes too low or the level of carbon dioxide in the blood becomes too high.
- Abnormal electrical conduction within the heart which could cause irregular heart beat, could cause the heart to stop beating and could be life-threatening
- Heart attack
- Damage to the liver which can lead to inflammation and/or scarring which could lead to a yellow appearance to the skin, and fluid collection in the abdomen (belly) which makes it look larger
- The liver rapidly loses its ability to function. This may cause many complications, including excessive bleeding and increasing pressure in the brain, requires hospitalization and may be life-threatening
- Severe blood infections which will need to be treated and may be life-threatening
- Convulsion (seizures)
- Severe kidney damage (which may be permanent)
- Severe rashes which can result in loss of skin and damage to mucous membranes and which may be life-threatening
mouth
- Tiny reddish or purplish spots containing blood that appears in skin or mucous membrane as a result of localized bleeding
- Abnormal low levels of magnesium in the body which may require that you take extra magnesium by mouth or vein
- High levels of sugar or calcium in the blood that may require treatment
- Pain in the joints, back and/or arms and legs
- Anxiety
- Confusional state
- Depression
- Difficulty sleeping or falling asleep
- Shortness of breath
- Low levels of oxygen in the blood which may make you feel short of breath
- A fast rate of respiration that may cause pain in the chest
- Nose bleed
- Inflammation of the pancreas (an organ in the abdomen which makes insulin and certain digestive chemicals). This may cause pain in the abdomen (belly) which can be severe and may increase the blood sugar.
- Enlarged liver
- The skin and the whites of the eyes appears yellow as a result of too much bilirubin (a substance that comes from the liver breaking down waste products) in the blood
- Blood in the urine which may indicate kidney (or bladder) damage
- Infection in the bladder or kidney
- Red bumpy rash which may become severe
Although caspofungin has the potential risks noted above, it may be better at preventing invasive fungal infections caused by Aspergillus as compared to fluconazole, but the benefit of caspofungin is uncertain.
For the optional studies, the greatest risk to you is the release of information from your health records. We will do our best to make sure that your personal information will be kept private. The chance that this information will be given to someone else is very small.
Are there benefits to taking part in the study?
We hope that this study will help you personally, but we do not know if it will.
Potential benefits to you could include a better chance of preventing invasive fungal infections during treatment for AML.
We expect that the information learned from this study will benefit other patients in the future.
What other options are there?
Instead of being in this study, you have these options:
Current standard therapy even if you do not take part in the study. Standard therapy is described on page 1. It is the Fluconazole Arm of this study.
Receiving no prevention against fungal infections.
Taking part in another study
Please talk to your doctor about these and other options.
How many people will take part in the study?
The total number of people enrolled on this study is expected to be 575.
How long is the study?
Subjects in this clinical trial are expected to receive treatment on this study for durations that will be determined by the length of your chemotherapy. After treatment, you will have follow-up examinations and medical tests.
We would like to continue to find out about your health for 2 years after you start this study.
You can stop taking part in the study at any time. However, if you decide to stop participating in the study, we encourage you to talk to the study doctor and your regular doctor first. They will help you stop safely.
Your doctor or the study doctor may decide to take you off this study:
if he/she believes that it is in your best interest
if your disease comes back during treatment
if you experience side effects from the treatment that are considered too severe
if new information becomes available that shows that another treatment would be better for you
What about privacy?
We will do our best to make sure that the personal information in your medical record will be kept private. However, we cannot guarantee total privacy. Your personal information may be given out if required by law. If information from this study is published or presented at scientific meetings, your name and other personal information will not be used.
The Children's Oncology Group has received a Certificate of Confidentiality from the federal government, which will help us protect the privacy of our research subjects. Information about the certificate is included in Attachment #3.
Organizations that may look at and/or copy your research or medical records for research, quality assurance and data analysis include groups such as:
The Children's Oncology Group
The Representatives of the National Cancer Institute (NCI), Food and Drug Administration (FDA), and other U.S. and international governmental regulatory agencies involved in overseeing research
The Institutional Review Board of this hospital
The Pediatric Central Institutional Review Board (CIRB) of the National Cancer Institute
The drug company that makes caspofungin or their designated reviewers.
What are the costs?
Taking part in this study may lead to added costs to you or your insurance company. There are no plans for the study to pay for medical treatment. Please ask about any expected added costs or insurance problems. Staff will be able to assist you with this.
In the case of injury or illness resulting from this study, emergency medical treatment is available but will be provided at the usual charge. No funds have been set aside to compensate you in the event of injury. However by signing this form, you are not giving up any legal rights to seek to obtain compensation for injury.
You or your insurance company will be charged for continuing medical care and/or hospitalization.
The drug company that makes caspofungin is supplying the drug at no charge for subjects on this study. Therefore, if you are randomized to the caspofungin arm, you or your insurance company will not be charged for the caspofungin. The drug company does not cover the cost of getting the caspofungin ready and giving it to you, so you or your insurance company may have to pay for this.
Caspofungin is given IV only. Therefore some hospitals may want to keep you admitted during the period you are receiving caspofungin, while others may discharge you to continue caspofungin at home. There may be additional costs to you or your insurance company if you are discharged from the hospital to continue to have the drug given at home. This may include the cost of caspofungin if given at home. If your insurance company or other hospital sources will not cover this additional cost and you cannot cover it yourself, you may stop taking caspofungin and use whatever your hospital usually uses to prevent fungal infections.
Fluconazole is a standard antifungal drug, and would most likely be given to you if you did not take part in the study. Therefore, if you are randomized to the fluconazole arm, you or your insurance company will be charged for the fluconazole.
For more information on clinical trials and insurance coverage, you can visit the National Cancer Institute's Web site at http://www.cancer.gov/clinicaltrials/learningabout. You can print a copy of the "Clinical Trials and Insurance Coverage" information from this Web site.
Funding support
If you choose to enroll on this study, this institution will receive some money from the Children's Oncology Group to do the research. There are no plans to pay you for taking part in this study.
The optional tests are not part of standard care. The cost of performing these tests will be free of charge. There will be no cost to you or your insurance company.
This study includes providing specimens to the researcher. There are no plans for you to profit from any new product developed from research done on your specimens.
What are my rights as a participant?
Taking part in this study is voluntary. You may choose not to be in this study. If you decide not to be in this study, you will not be penalized and you will not lose any benefits to which you are entitled. You will still receive medical care.
You can decide to stop being in the study at any time. Leaving the study will not result in any penalty or loss of benefits to which you are entitled. Your doctor will still take care of you.
We will tell you about new information that may affect your health, welfare, or willingness to stay in this study. A committee outside of COG closely monitors study reports and notifies COG if changes must be made to the study. Members of COG meet twice a year to discuss results of treatment and to plan new treatments.
During your follow-up visits after treatment, you may ask to be given a summary of the study results after they are written up. This may be several years from now since all people on the study need to have completed treatment.
Whom do I call if I have questions or problems?
For questions about the study or if you have a research related problem or if you think you have been injured in this study, you may contact Dr. XXXX or your doctor at XXXXX.
If you have any questions about your rights as a research participant or any problems that you feel you cannot discuss with the investigators, you may call XXXX IRB Administrator at XXXX.
If you have any questions or concerns that you feel you would like to discuss with someone who is not on the research team, you may also call the Patient Advocate at XXXX.
Where can I get more information?
The COG Family Handbook for Children with Cancer has information about specific cancers, tests, treatment side effects and their management, adjusting to cancer, and resources. Your doctor can get you this Handbook, or you can get it at http://www.childrensoncologygroup.org/familyhandbook.
Visit the NCI's Web site at http://www.cancer.gov.
If you are in the United States, you may call the NCI's Cancer Information Service at: 1-800-4-CANCER (1-800-422-6237).
A description of this clinical trial will be available at: http://www.ClinicalTrials.gov, as required by U.S. Law. This web site will not include information that can identify you. At most, the web site will include a summary of the results. You can search this web site at any time.
You will get a copy of this form. You may also ask for a copy of the protocol (full study plan).
Specimens for optional research tests
This section of the informed consent is about samples for the optional research tests (biomarker and SNP studies).
The choice to let us use specimens for research is up to you. No matter what you decide to do, it will not affect your care. You can still be a part of the main study even if you say 'No' to taking part in any of these optional research studies.
If you decide now that your specimens can be used for research and banking you can change your mind at any time. Just contact us and let us know that you do not want us to use your specimens. Then any specimens that we have will be destroyed.
If you want to learn more about tissue research with banked specimens, the NCl website has an information sheet called "Providing Your Tissue For Research: What You Need To Know." This sheet can be found at: http://www.cancer.gov/clinicaltrials/resources/providingtissue.
Please read the information below and think about your choices. After making your decisions, check "Yes" or "No", then add your initials and the date after your answer. If you have any questions, please talk to your doctor or nurse, or call our research review board at the IRB's phone number included in this consent.
I agree to the collection of extra blood samples for the research studies about biomarkers in the blood that may show fungal infections as early as possible.
Yes No 1
Initials
Date
[For Subjects Enrolled on AAML1031]
I agree that a blood sample (currently in a COG laboratory) may be used to look at genetic risk factors for fungal infections.
Yes
No
[For Subjects NOT Enrolled on AAML 1031]
2. I agree to the collection of extra blood for SNP analysis that will look at genetic risk factors for fungal infections.
Yes
No 1
Initials
Date
3. If some blood is left over after the studies above are completed, I agree that it may be kept (banked) for future research to learn about, prevent, or treat cancer.
Yes No /
Initials
Date
4. If some blood is left over after the studies above are completed, I agree that it may be kept (banked) for use in research to learn about, prevent or treat other health problems (for example: diabetes, Alzheimer's disease, or heart disease).
Yes No /
Initials
Date
SIGNATURE
I have been given a copy of all pages of this form. The form includes three (3) attachments.
I have reviewed the information and have had my questions answered.
I agree to take part in this study (ACCL0933)
Participant Date
Parent/Guardian Date
Parent/Guardian Date
Physician/PNP obtaining consent Date
IRB#
IRB Approved:
Attachment #1
Treatment and Procedures Common to all Patients at Risk of IFI
Method for Giving Drugs
IV - Drug is given using a needle or tubing inserted into a vein. Drugs can be given rapidly over a few minutes ("push") or slowly over minutes or hours ("infusion").
PO- Drug is given by tablet or liquid swallowed through the mouth.
Central Line
Your doctor may recommend that you get a special kind of IV called a "central line." This is a kind of IV placed into a big vein in your chest that can stay in for a long time. The risks associated with central lines will be explained to you and all of your questions will be answered. If you are to have a central line inserted, you will be given a separate informed consent document to read and sign for this procedure. A description of the types of central lines is in the COG Family Handbook for Children with Cancer.
Therapy for Patient on Fluconazole Treatment Plan (Standard Treatment Arm)
The purpose of fluconazole therapy is to prevent the development of invasive fungal infections following treatment with chemotherapy for AML.
Drug
How the drug will be
given
Days
Fluconazole
IV infusion over 1-2 hours
(or longer) or PO
Once a day*
*Start at the end of each chemotherapy course & continue until blood cells recover or the next chemotherapy course begins.
Standard Tests and Procedures
The following tests and procedures are part of regular cancer care and may be done even if you do not join the study.
History and physical exam.
Frequent labs to monitor blood counts and blood chemistries.
Urine tests to measure how the kidneys are functioning.
Pregnancy test for females of childbearing age before treatment begins.
Attachment #2
Risks of Drugs Used to Prevent Invasive Fungal Infections
Risks and side effects related to fluconazole include:
Likely
May happen in 21 to 100 subjects out of every 100
Less Likely
May happen in 20 or less than 20 subjects out of every 100
Rare but serious
- Allergic reaction
- Shortness of breath
- Nausea and/or vomiting
- Bloating
- Acid or upset stomach (heartburn)
- Change in taste
- Diarrhea
- Abdominal pain
- Headache
- Dizziness (rare)
- Skin rash
- Itching
- Low level of potassium in the blood which may cause weakness, tiredness, muscle cramps, constipation, and abnormal heart beat and may require that you take extra potassium by mouth or through the vein
- Increase of triglycerides and cholesterol in the blood which could lead to heart problems later in life
- A rare but severe lowering of the white blood cell count which can make you very susceptible to infections which could be lifethreatening
- An increase in the blood of a type of white blood cell called an eosinophil. These are sometimes associated with allergic reactions.
- A low number of platelets causes you to bruise and bleed more easily
- Increase in the blood of certain enzymes which could indicate liver irritation or damage
- A condition in which the flow of bile from the liver is blocked and may cause itching, dark colored urine, light colored feces, and yellow eyes or skin
- Hair loss with prolonged fluconazole use
- Severe allergic reaction which can be life-threatening with shortness of breath, low blood pressure, rapid heart rate, chills and fever
- A heart rhythm disorder that can cause fast, chaotic heartbeats. The rapid heartbeats may lead to fainting and in some cases, your heart's rhythm may beat so erratically that it can be life-threatening
- Severe rashes which can result in loss of skin and damage to mucous membranes and which may be lifethreatening
- Seizures (convulsions)
- Damage to the liver which can lead to inflammation and/or scarring which could lead to a yellow appearance to the skin, and fluid collection in the abdomen (belly) which makes it look larger
- The liver rapidly loses its ability to function. This may cause many complications, including excessive bleeding and increasing pressure in the brain, requires hospitalization and may be lifethreatening
Attachment #3
Certificate of Confidentiality
The Children's Oncology Group has received a Certificate of Confidentiality from the federal government, which will help us protect the privacy of our research subjects. The Certificate protects against the involuntary release of information about subjects collected during the course of our covered studies. The researchers involved in the studies cannot be forced to disclose the identity or any information collected in the study in any legal proceedings at the federal, state, or local level, regardless of whether they are criminal, administrative, or legislative proceedings. However, the subject or the researcher may choose to voluntarily disclose the protected information under certain circumstances. For example, if the subject or his/her guardian requests the release of information in writing, the Certificate does not protect against that voluntary disclosure. Furthermore, federal agencies may review our records under limited circumstances, such as a DHHS request for information for an audit or program evaluation or an FDA request under the Food, Drug and Cosmetics Act.
The Certificate of Confidentiality will not protect against the required reporting by hospital staff of information on suspected child abuse, reportable communicable diseases, and/or possible threat of harm to self or others.
*Protocol therapy must begin within 24-72 hours following the completion of the first course of systemic chemotherapy for current diagnosis. Prophylaxis started within 24-72 hours following completion of each systemic chemotherapy course and continues until ANC following the nadir. Galactomannan and beta-D glucan testing twice weekly. See Section 13 for details. SNP- Single Nucleotide Polymorphisms. Collect sample at end of Course 1. See Section 14 for details. IFI-Invasive Fungal Infections (including Invasive Aspergillosis)
HSCT - Hematopoietic Stem Cell Transplantation
*Based on median duration of neutropenia for each course from AAML0531 trial Based on a plan for 2 tests per week during neutropenic period
If culture is available, append the identification at the genus or species level from the culture results. Tissue and cells submitted for histopathologic or cytopathologic studies should be stained by Grocott-Gomorri methenamine silver stain or by periodic acid Schiff stain, to facilitate inspection of fungal structures. Whenever possible, wet mounts of specimens from foci related to invasive fungal disease should be stained with a fluorescent dye (e.g., calcofluor or blankophor). Candida, Trichosporon, and yeast-like Geotrichum species and Blastoschizomyces capitatus may also form pseudohyphae or true hyphae. Recovery of Aspergillus species from blood cultures invariably represents contamination
NOTE. Probable IFD requires the presence of a host factor, a clinical criterion, and a mycological criterion. Cases that meet the criteria for a host factor and a clinical criterion but for which mycological criteria are absent are considered possible IFD. Host factors are not synonymous with risk factors and are characteristics by which individuals predisposed to invasive fungal diseases can be recognized. They are intended primarily to apply to patients given treatment for malignant disease and to recipients of allogeneic hematopoietic stem cell and solid-organ transplants. These host factors are also applicable to patients who receive corticosteroids and other T cell suppressants as well as to patients with primary immunodeficiencies. Must be consistent with the mycological findings, if any, and must be temporally related to current episode. Every reasonable attempt should be made to exclude an alternative etiology. The presence of signs and symptoms consistent with sepsis syndrome indicates acute disseminated disease, whereas their absence denotes chronic disseminated disease. These tests are primarily applicable to aspergillosis and candidiasis and are not useful in diagnosing infections due to Cryptococcus species or Zygomycetes (e.g., Rhizopus, Mucor, or Absidia species). Detection of nucleic acid is not included, because there are as yet no validated or standardized methods.